|
|
|
| Cytoreductive radical prostatectomy after chemohormonal therapy in patients with primary metastatic prostate cancer |
Christa Babsta,Thomas Amiela,Tobias Maurerb,Sophie Knipperb,Lukas Lungera,Robert Taubera,Margitta Retza,Kathleen Herkommera,Matthias Eibera,Gunhild von Amsbergb,Markus Graefenb,Juergen Gschwenda,Thomas Steuberb,Matthias Hecka,*( ) )
|
a Department of Urology, Technical University of Munich, Rechts der Isar Medical Center, Munich, Germany
b Martini-Klinik Prostate Cancer Center, Hamburg, Germany |
|
|
|
|
Abstract Objective: Cytoreductive radical prostatectomy (cRP) has been proposed as local treatment option in metastatic hormone-sensitive prostate cancer (mHSPC) to prevent local complications and potentially improve oncological outcomes. In this study, we examined the feasibility of a multimodal concept with primary chemohormonal therapy followed by cRP and analyzed prostate size reduction under systemic treatment, postoperative complication rates, as well as early postoperative continence.
Methods: In this retrospective study, 38 patients with mHSPC underwent cRP after primary chemohormonal therapy (3-monthly luteinising hormone-releasing hormone-analogue + six cycles 3-weekly docetaxel 75 mg/m2) at two centers between September 2015 and December 2018.
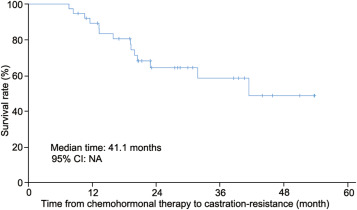
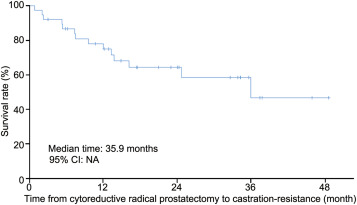
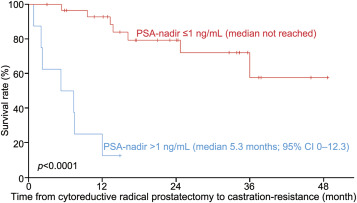
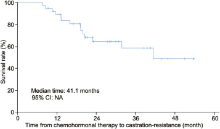
Results: Overall, 10 (26%) patients had high volume and 28 (74%) patients had low volume disease at diagnosis, according to CHAARTED definition. Median prostate-specific antigen (PSA) decreased from 65 ng/mL (interquartile range [IQR] 35.0-124.5 ng/mL) pre-chemotherapy to 1 ng/mL (IQR 0.3-1.7 ng/mL) post-chemotherapy. Prostate gland volume was significantly reduced by a median of 50% (IQR 29%-56%) under chemohormonal therapy (p = 0.003). Postoperative histopathology showed seminal vesicle invasion in 33 (87%) patients and negative surgical margins in 17 (45%) patients. Severe complications (Grade 3 according to Clavien-Dindo) were observed in 4 (11%) patients within 30 days. Continence was reached in 87% of patients after 1 month and in 92% of patients after 6 months. Median time to castration-resistance from begin of chemohormonal therapy was 41.1 months and from cRP was 35.9 months. Postoperative PSA-nadir ≤1 ng/mL versus >1 ng/mL was a significant predictor of time to castration-resistance after cRP (median not reached versus 5.3 months; p<0.0001).
Conclusion: We observed a reduction of prostate volume under chemohormonal therapy going along with a low postoperative complication and high early continence rate. However, the oncologic benefit from cRP is still under evaluation.
|
|
Received: 30 May 2020
Available online: 20 January 2022
|
|
Corresponding Authors:
Matthias Heck
E-mail: matthias.heck@tum.de
|
|
|

| Characteristic | Value | | Age, median (IQR), year | 57 (54-64) | | Number of patients, n (%) | | ≥65 years | 9 (23) | | <65 years | 29 (77) | | ASA score, median (IQR) | 2 (2-2) | | PSA, median (IQR), ng/mL | | At diagnosis | 65 (35.0-124.5) | | Pre-surgery | 1.0 (0.3-1.7) | | Gleason score, n | | 6 | 1 | | 7a | 2 | | 7b | 2 | | 8 | 9 | | 9 | 21 | | 10 | 3 | | Median (IQR) | 9 (8-9) | | CHAARTED criteria, n (%) | | Low volume disease | 28 (74) | | High volume disease | 10 (26) | | Metastases status at diagnosis, n (%) | | Lymph node | 33 (87) | | Bone | 23 (61) | | Visceral | 2 (5) | | Time from diagnosis to chemotherapy, median (IQR), day | 53 (32-74) | | Time from diagnosis to surgery, median (IQR), day | 250 (222-281) | | Time from end of chemotherapy to surgery, median (IQR), day | 61 (47-82) | | Prostate volume, median (IQR), mL | | Pre-docetaxel | 50 (35-64) | | Pre-surgery | 25 (15-31) | | Prostate volume reduction, median (IQR), mL | 25 (10-35) | | Prostate volume reduction, median (IQR), % | 50 (29-56) | | Hemoglobin, median (IQR), g/dL | | Pre-surgery | 13.7 (13.0-14.1) | | Post-surgery (Day 1 after surgery) | 10.7 (10.2-12.1) | | Hemoglobin loss, median (IQR), g/dL | 2.9 (1.9-3.4) | | Operation time, median (IQR), min | 196 (157-233) | | Hospital length of stay, median (IQR), day | 9 (6-10) | | Postoperative T stage, n (%) | | pT2c | 2 (5) | | pT3a | 3 (8) | | pT3b | 33 (87) | | Postoperative N stage, n (%) | | pN0 | 4 (11) | | pN1 | 34 (89) | | Lymph nodes removed, median (IQR), n | 18.5 (12-24) | | Positive lymph nodes, median (IQR), n | 3 (1-6) | | Margin status, n (%) | | R0 | 17 (45) | | R1 | 21 (55) |
|
|
Descriptive characteristics of 38 patients treated with cytoreductive radical prostatectomy after chemohormonal therapy.
|
|
|
Kaplan-Meier curve showing the time from begin of chemohormonal therapy to development of castration resistance. NA, not available; CI, confidence interval.
|

|
|
Kaplan-Meier curve showing the time from cytoreductive prostatectomy to development of castration resistance. CI, confidence interval; NA, not available.
|

|
|
Kaplan-Meier curve showing the time from cytoreductive prostatectomy to development of castration resistance stratified by postoperative PSA-nadir ≤1 ng/mL versus >1 ng/mL.CI, confidence interval.
|
| Pad use | Postoperative continence after 1 month (n=31a), n (%) | Postoperative continence after 6 months (n=25b), n (%) | Postoperative continence after 12 months (n=26c), n (%) | | 0 pad | 2 (6) | 15 (60) | 18 (69) | | 1 pad (for security) | 25 (81) | 8 (32) | 5 (19) | | 1 wet pad (mild incontinence) | 1 (3) | 1 (4) | 1 (4) | | 2 wet pads (moderate incontinence) | 3 (10) | 1 (4) | 2 (8) | | ≥3 pads (severe incontinence) | 0 | 0 | 0 |
|
|
Continence and pad use.
|
| [1] |
Heidenreich A, Bastian PJ, Bellmunt J, Bolla M, Joniau S, van der Kwast T, et al. EAU guidelines on prostate cancer Part II: Treatment of advanced, relapsing, and castration-resistant prostate cancer. Eur Urol 2014; 65:467e79.
|
| [2] |
Sweeney CJ, Chen YH, Carducci M, Liu G, Jarrard DF, Eisenberger M, et al. Chemohormonal therapy in metastatic hormone-sensitive prostate cancer. N Engl J Med 2015; 373:737e46.
|
| [3] |
James ND, Sydes MR, Clarke NW, Mason MD, Dearnaley DP, Spears MR, et al. STAMPEDE investigators. Addition of docetaxel, zoledronic acid, or both to first-line long-term hormone therapy in prostate cancer (STAMPEDE): Survival results from an adaptive, multiarm, multistage, platform randomised controlled trial. Lancet 2016; 387:1163e77.
|
| [4] |
Tzelepi V, Efstathiou E, Wen S, Troncoso P, Karlou M, Pettaway CA, et al. Persistent, biologically meaningful prostate cancer after 1 year of androgen ablation and docetaxel treatment. J Clin Oncol 2011; 29:2574e81.
|
| [5] |
Gundem G, Van Loo P, Kremeyer B, Alexandrov LB, Tubio JMC, Papaemmanuil E, et al. The evolutionary history of lethal metastatic prostate cancer. Nature 2015; 520:353e7.
|
| [6] |
Culp SH, Schellhammer PF, Williams MB. Might men diagnosed with metastatic prostate cancer benefit from definitive treatment of the primary tumor? A SEER-based study. Eur Urol 2014; 65:1058e66.
|
| [7] |
Gratzke C, Engel J, Stief CG. Role of radical prostatectomy in metastatic prostate cancer: Data from the Munich Cancer Registry. Eur Urol 2014; 66:602e3.
|
| [8] |
Leyh-Bannurah SR, Gazdovich S, Budäus L, Zaffuto E, Briganti A, Abdollah F, et al. Local therapy improves survival in metastatic prostate cancer. Eur Urol 2017; 72:118e24.
|
| [9] |
Steuber T, Berg KD, Røder MA, Brasso K, Iversen P, Huland H, et al. Does cytoreductive prostatectomy really have an impact on prognosis in prostate cancer patients with low-volume bone metastasis? Results from a prospective case-control study. Eur Urol Focus 2017; 3:646e9.
|
| [10] |
Heidenreich A, Pfister D, Porres D. Cytoreductive radical prostatectomy in patients with prostate cancer and low volume skeletal metastases: Results of a feasibility and casecontrol study. J Urol 2015; 193:832e8.
|
| [11] |
Heidenreich A, Fossati N, Pfister D, Suardi N, Montorsi F, Shariat S, et al. Cytoreductive radical prostatectomy in men with prostate cancer and skeletal metastases. Eur Urol Oncol 2018: 46e53.
|
| [12] |
Mitropoulos D, Artibani W, Biyani CS, Bjerggaard Jensen J, Roupreêt M, Truss M. Validation of the Clavien-Dindo grading system in urology by the European Association of Urology guidelines ad hoc panel. Eur Urol Focus 2018; 4:608e13.
|
| [13] |
Mottet N, Bellmunt J, Bolla M, Briers E, Cumberbatch MG, De Santis M, et al; Members of the EAUeESTROeESUReSIOG prostate cancer guidelines panel. EAUeESTROeESUReSIOG Guidelines on Prostate Cancer. [Accessed 15 August 2020]. https://uroweb.org/guideline/prostate-cancer/.
|
| [14] |
Pompe RS, Beyer B, Haese A, Preisser F, Michl U, Steuber T, et al. Postoperative complications of contemporary open and robot-assisted laparoscopic radical prostatectomy using standardised reporting systems. BJU Int 2018; 122:801e7.
|
| [15] |
Michl U, Tennstedt P, Feldmeier L, Mandel P, Oh SJ, Ahyai S, et al. Nerve-sparing surgery technique, not the preservation of the neurovascular bundles, leads to improved long-term continence rates after radical prostatectomy. Eur Urol 2016; 69:584e9.
|
| [16] |
Pompe RS, Karakiewicz PI, Tian Z, Mandel P, Steuber T, Schlomm T, et al. Oncological and functional outcome after radical prostatectomy for high or very high-risk prostate cancer: European validation of the current NCCN_ guideline. J Urol 2017; 198:354e61.
|
| [17] |
Kyriakopoulos CE, Chen YH, Carducci MA, Liu G, Jarrard DF, Hahn NM, et al. Chemohormonal therapy in metastatic hormone-sensitive prostate cancer: Long-term survival analysis of the randomized phase III E3805 CHAARTED trial. J Clin Oncol 2018; 36:1080e7.
|
| [18] |
Clarke NW, Ali A, Ingleby FC, Hoyle A, Amos CL, Attard G, et al. Addition of docetaxel to hormonal therapy in low- and high-burden metastatic hormone sensitive prostate cancer: Long-term survival results from the STAMPEDE trial. Ann Oncol 2019; 30:1992e2003.
|
| [19] |
Gravis G, Boher JM, Chen YH, Liu G, Fizazi K, Carducci MA, et al. Burden of metastatic castrate naive prostate cancer patients, to identify men more likely to benefit from early docetaxel: Further analyses of CHAARTED and GETUG-AFU15 studies. Eur Urol 2018; 73:847e55.
|
| [20] |
Fizazi K, Tran N, Fein L, Matsubara N, Rodriquez-Antolin A, Alekseev BY, et al. LATITUDE Investigators. Abiraterone plus prednisone in metastatic, castration-sensitive prostate cancer. N Engl J Med 2017; 377:352e60.
|
| [21] |
Armstrong AJ, Szmulewitz RZ, Petrylak DP, Holzbeierlein J, Villers A, Azad A, et al. ARCHES: A randomized, phase III study of androgen deprivation therapy with enzalutamide or placebo in men with metastatic hormone-sensitive prostate cancer. J Clin Oncol 2019; 37:2974e86.
|
| [22] |
Davis ID, Martin AJ, Stockler MR, Begbie S, Chi KN, Chowdhury S, et al. Enzalutamide with standard first-line therapy in metastatic prostate cancer. N Engl J Med 2019; 381:121e31.
|
| [23] |
Chi KN, Agarwal N, Bjartell A, Chung BH, Pereira de Santana Gomes AJ, Given R, et al. Apalutamide for metastatic, castration-sensitive prostate cancer. N Engl J Med 2019; 381:13e24.
|
| No related articles found! |
|
|
|
|