|
|
|
| Perioperative anticoagulation and open distal corpora cavernosa shunt in the management of a case of stuttering idiopathic persistent childhood ischaemic priapism |
Jonathan S.M. Teoa,b,Han Jie Leeb,John S.P. Yuenb,*( ) )
|
a Department of Urology, Sengkang General Hospital, Singapore
b Department of Urology, Singapore General Hospital, Singapore |
|
|
|
|
Abstract Childhood priapism is a rare entity and there is currently no consensus regarding its contemporary management. The use of perioperative anticoagulation and open distal corpora-glandular shunt procedure in the management of childhood priapism has not been reported in the literature. We present a stuttering case of a 13-year-old boy who presented with idiopathic ischaemic priapism lasting 13 h in duration, which recurred despite corporal aspiration and alpha-adrenergic agonist injections, percutaneous distal shunt surgery, and revision of percutaneous distal shunt surgery. He was eventually successfully managed with perioperative subcutaneous enoxaparin, oral aspirin and clopidogrel in conjunction with an Al-Ghorab shunt, which led to sustained detumescence but with spontaneous morning erections. In paediatric patients with sustained childhood priaprism failing stepwise treatments, an Al-Ghorab shunt with perioperative anticoagulation is a viable option.
|
|
Received: 02 June 2019
Available online: 30 December 2019
|
|
Corresponding Authors:
John S.P. Yuen
E-mail: john.yuen.s.p@singhealth.com.sg
|
|
|

|
|
Aspiration of dark red blood using large bore 18-gauge butterfly needle inserted at the peno-scrotal junction at 9 o'clock position.
|

|
|
Bilateral percutaneous distal T shunt after closure of incisions on glans penis.
|
|
|
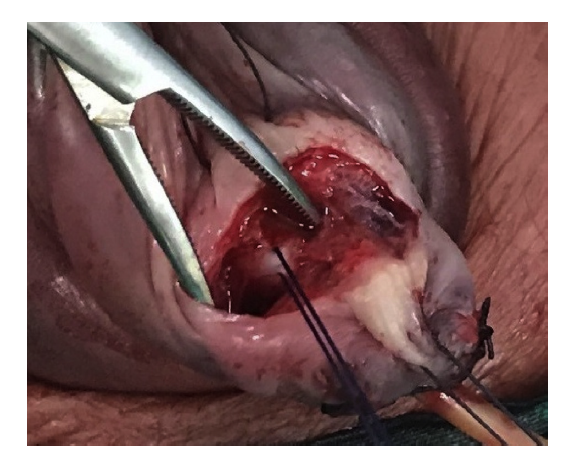
Open distal Al-Ghorab shunt with the white tunica albuginea layer covering the corpora cavernosa.
|
| [1] |
Donaldson JF, Rees RW, Steinbrecher HA. Priapism in children: A comprehensive review and clinical guideline. J Pediatr Urol 2014; 10:11e24.
|
| [2] |
Montague DK, Jarow J, Broderick GA, Dmochowski RR, Heaton JP, Lue TF, et al. American Urological Association guideline on the management of priapism. J Urol 2003; 170:1318e24.
|
| [3] |
Broderick GA, Kadioglu A, Bivalacqua TJ, Ghanem H, Nehra A, Shamloul R. Priapism: Pathogenesis, epidemiology, and man-agement. J Sex Med 2010; 7:476e500.
|
| [4] |
Lue TF, Pescatori ES. Distal cavernosum-glans shunts for ischemic priapism. J Sex Med 2006; 3:749e52.
|
| [5] |
Ercole CJ, Pontes JE, Pierce JM. Changing surgical concepts in the treatment of priapism. J Urol 1981; 125:210e1.
|
| [6] |
Lue TF, Garcia M. Should perioperative anticoagulation be an integral part of the priapism shunting procedure? Transl Androl Urol 2013; 2:316e20.
|
| [7] |
Kulmala RV, Lehtonen TA, Tammela TL. Priapism, its incidence and seasonal distribution in Finland. Scand J Urol Nephrol 1995; 29:93e6.
|
| [8] |
Eland IA, van der Lei J, Stricker BH, Sturkenboom MJ. Inci-dence of priapism in the general population. Urology 2001; 57:970e2.
|
| [9] |
Burnett AL, Bivalacqua TJ. Priapism: New concepts in medical and surgical management. Urol Clin N Am 2011; 38:185e94.
|
| [10] |
Furtado PS, Costa MP, Ribeiro do Prado Valladares F, Oliveira da Silva L, Lordêlo M, Lyra I, et al. The prevalence of priapism in children and adolescents with sickle cell disease in Brazil. Int J Hematol 2012; 95:648e51.
|
| [11] |
Tarry WF, Duckett JW, Snyder HM. Urological complications of sickle cell disease in a pediatric population. J Urol 1987; 138:592e4.
|
| [12] |
Dewan PA, Tan HL, Auldist AW, Moss DI. Priapism in childhood. Br J Urol 1989; 64:541e5.
|
|
|
|