|
|
|
| Oncological outcomes of patients with ductal adenocarcinoma of the prostate receiving radical prostatectomy or radiotherapy |
Mengzhu Liua,Kun Jina,Shi Qiua,b,Pengyong Xuc,Mingming Zhanga,Wufeng Caia,Xiaonan Zhenga,Lu Yanga,*( ),Qiang Weia ),Qiang Weia
|
a Institute of Urology, Department of Urology, West China Hospital, Sichuan University, Chengdu, China
b Center of Biomedical Big Data, West China Hospital, Sichuan University, Chengdu, China
c Institute of Urology, Department of Urology, the First People’s Hospital, Yantai, China |
|
|
|
|
Abstract Objective To evaluate the oncological outcomes of ductal adenocarcinoma of the prostate (DAC) managed with radical prostatectomy (RP) or radiotherapy (RT) and optimize the proper treatment modality to DAC comprehensively.
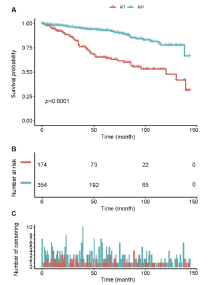
Methods The cohorts included a total of 528 patients from the Surveillance, Epidemiology and End Results (SEER) database, 354 receiving RP and 174 receiving RT. Cox proportional hazards regressions were performed to assess cancer specific mortality (CSM) and overall mortality (OM) between treatment groups. A competing risk analysis was further conducted. Subgroup analyses by age and level of prostate-specific antigen (PSA) were performed. Propensity score matching was implemented.
Results Patients managed with RP had lower risks of CSM and OM compared with RT (before matching: Hazard ratio [HR]=0.24, 95% confidence interval [CI] 0.13-0.47 and HR=0.26, 95% CI 0.17-0.40, respectively; after matching: HR=0.18, 95% CI 0.04-0.82 and HR=0.28, 95% CI 0.11-0.70, accordingly). Subgroup analyses demonstrated that patients in the middle tertile of the age or with lower tertile PSA level managed with RP took lower risks of OM significantly (HR=0.18, 95% CI 0.06-0.57, p<0.01 and HR=0.17, 95% CI 0.06-0.54, p<0.01).
Conclusion Among patients with DAC, treatment with RP was associated with better survival outcomes in comparison with RT. Patients with DAC in the middle tertile of the age and with lower tertile PSA level benefited the most from RP.
|
|
Received: 24 July 2019
Available online: 23 May 2020
|
|
Corresponding Authors:
Lu Yang
E-mail: wycleflue@163.com
|
|
|

| RT (n=174) | RP (n=354) | p-Value | | Age, year | | | | | mean±SD | 71.51±8.26 | 63.64±8.26 | <0.01 | | median (IQR) | 72.50 (67.00-77.00) | 63.00 (58.25-69.00) | | | PSA level, ng/mL | | | | | mean±SD | 17.78±27.02 | 11.85±19.40 | 0.01 | | median (IQR) | 6.75 (4.35-15.58) | 6.10 (4.40-9.40) | | | Time, month | | | | | mean±SD | 50.63±36.96 | 57.86±39.66 | 0.05 | | median (IQR) | 43.00 (20.00-77.50) | 55.00 (23.00-85.00) | | | Marital status, n (%) | | Married | 118 (67.82) | 275 (77.69) | 0.03 | | Single | 12 (6.90) | 27 (7.63) | | Divorced/widowed | 30 (17.24) | 32 (9.04) | | Unknown | 14 (8.05) | 20 (5.65) | | Race, n (%) | | Caucasian | 131 (75.29) | 278 (78.53) | 0.52 | | African | 26 (14.94) | 44 (12.43) | | Other | 15 (8.62) | 31 (8.76) | | Unknown | 2 (1.15) | 1 (0.28) | | Clinical T stage, n (%) | | T1 | 75 (43.10) | 2 (0.57) | <0.01 | | T2 | 55 (31.61) | 166 (46.89) | | T3 | 24 (13.79) | 157 (44.35) | | T4 | 15 (8.62) | 29 (8.19) | | Unknown | 5 (2.87) | 0 (0.00) | | N stage, n (%) | | N0 | 157 (90.23) | 326 (92.09) | 0.01 | | N1 | 8 (4.60) | 26 (7.35) | | Unknown | 9 (5.17) | 2 (0.57) | | M stage, n (%) | | M0 | 151 (86.78) | 350 (98.87) | <0.01 | | M1 | 20 (11.49) | 3 (0.85) | | Unknown | 3 (1.72) | 1 (0.28) | | Biopsy Gleason grade group, n (%) | | I | 2 (1.15) | 1 (0.28) | <0.01 | | II | 19 (10.92) | 68 (19.21) | | III | 118 (67.82) | 266 (75.14) | | IV | 1 (0.57) | 3 (0.85) | | Unknown | 34 (19.54) | 16 (4.52) | | Biopsy gleason score, n (%) | | 6 | 20 (11.49) | 37 (10.45) | 0.01 | | 7 | 9 (5.17) | 50 (14.12) | | 8 | 31 (17.82) | 44 (12.43) | | Unknown | 114 (65.52) | 223 (62.99) |
|
|
Baseline characteristics of patients with DAC.
|
| CSM | OM | | HR (95% CI) | p-Value | HR (95% CI) | p-Value | | Non-adjusted (n=528) | | RT | 1 | | 1 | | | RP vs. RT | 0.24 (0.13, 0.47) | <0.01 | 0.26 (0.17, 0.40) | <0.01 | | Adjusted (n=487)a | | RT | 1 | | 1 | | | RP vs. RT | 0.41 (0.17, 0.99) | 0.05 | 0.50 (0.28, 0.90) | 0.02 |
|
|
Cox proportional hazards regression models of CSM and OM.
|
|
|
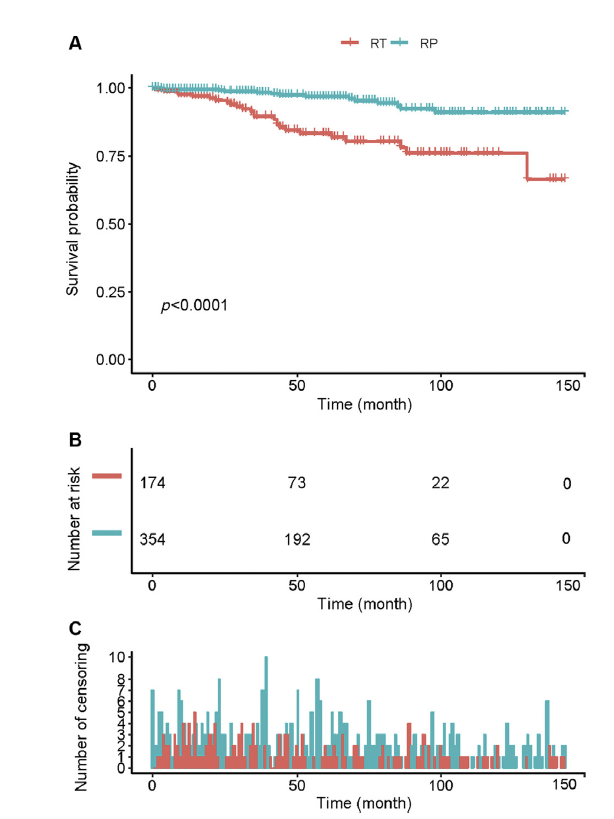
Kaplan-Meier analyses depicting cancer-specific mortality rates. (A) Survival curves; (B) Number at risk at different times; (C) Number of censoring at different times. RT, radiotherapy; RP, radical prostatectomy.
|
|
|
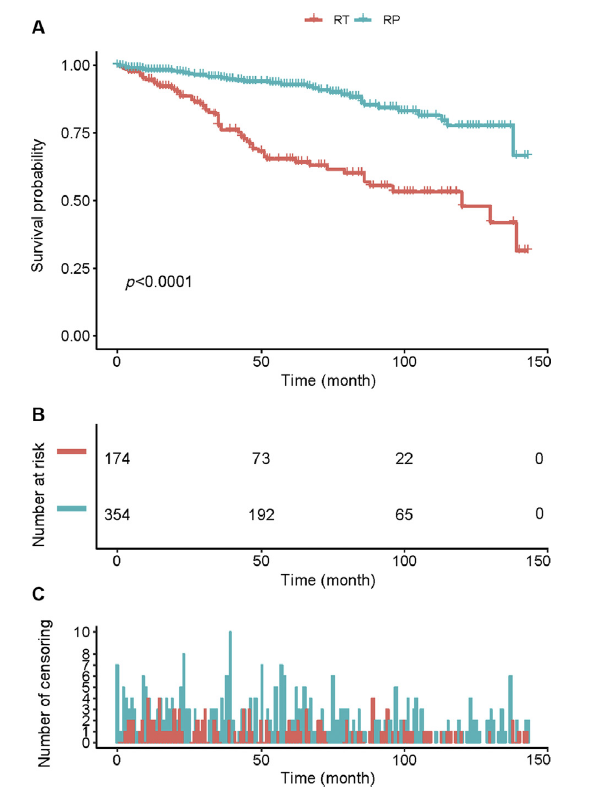
Kaplan-Meier analyses depicting overall mortality rates. (A) Survival curves; (B) Number at risk at different times; (C) Number of censoring at different times. RT, radiotherapy; RP, radical prostatectomy.
|
|
|
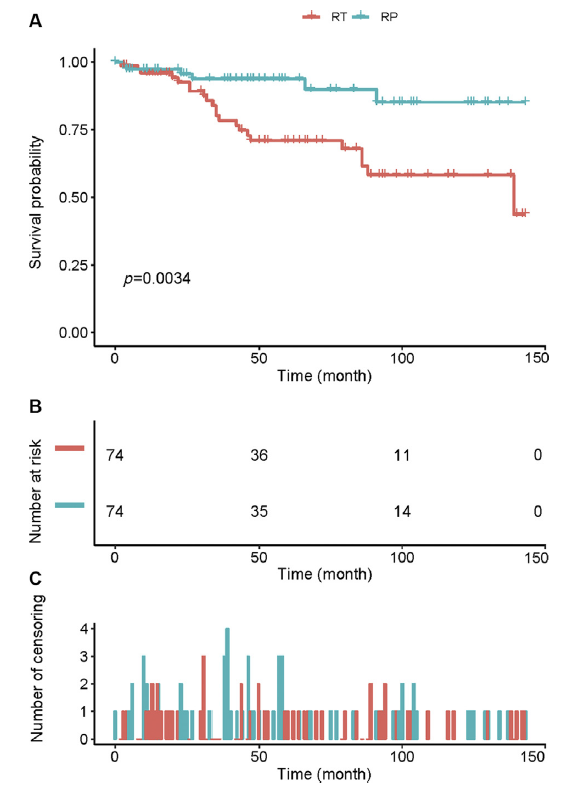
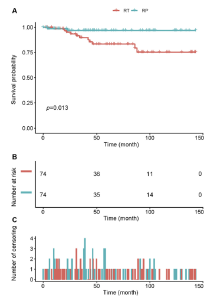
Kaplan-Meier analyses depicting cancer-specific mortality rates after propensity score matching. (A) Survival curves; (B) Number at risk at different times; (C) Number of censoring at different times. RT, radiotherapy; RP, radical prostatectomy.
|
|
|
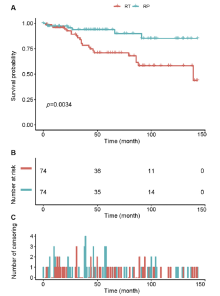
Kaplan-Meier analyses depicting overall mortality rates after propensity score matching. (A) Survival curves; (B) Number at risk at different times; (C) Number of censoring at different times. RT, radiotherapy; RP, radical prostatectomy.
|
| CSM | OM | | HR (95% CI), RP vs. RT | p-Value | HR (95% CI), RP vs. RT | p-Value | | Age a | | Low (n=157) | 0.10 (0.00, 37.88) | 0.44 | 0.10 (0.00, 37.88) | 0.44 | | Middle (n=180) | 0.08 (0.01, 0.71) | 0.02 | 0.18 (0.06, 0.57) | <0.01 | | High (n=191) | 0.52 (0.12, 2.16) | 0.36 | 0.61 (0.28, 1.31) | 0.20 | | PSA level b | | Low (n=161) | 0.16 (0.02, 1.21) | 0.08 | 0.17 (0.06, 0.54) | <0.01 | | Middle (n=158) | 0.07 (0.00, 1.58) | 0.09 | 1.16 (0.32, 4.27) | 0.82 | | High (n=168) | 0.79 (0.21, 2.92) | 0.72 | 0.67 (0.26, 1.76) | 0.42 |
|
|
Subgroup analyses by age and PSA level.
|
| RT (n=74) | RP (n=74) | p-Value | | Age, year | | | | | mean±SD | 68.70±7.99 | 67.28±10.65 | 0.36 | | median (IQR) | 70.00 (65.00-74.00) | 69.00 (62.25-74.00) | | | PSA level, ng/mL | | | | | mean±SD | 16.11±24.42 | 15.36±25.29 | 0.86 | | median (IQR) | 7.25 (4.40-14.88) | 5.80 (3.38-13.73) | | | Time, month | | | | | mean±SD | 56.81±39.52 | 55.49±39.43 | 0.84 | | median (IQR) | 47.00 (23.00-87.50) | 46.50 (23.25-89.00) | | | Marital status, n (%) | | Married | 52 (70.27) | 53 (71.62) | 0.49 | | Single | 6 (8.11) | 4 (5.41) | | Divorced/widowed | 13 (17.57) | 10 (13.51) | | Unknown | 3 (4.05) | 7 (9.46) | | Race, n (%) | | Caucasian | 53 (71.62) | 59 (79.73) | 0.39 | | African | 14 (18.92) | 8 (10.81) | | Other | 7 (9.46) | 6 (8.11) | | Unknown | 0 (0.00) | 1 (1.35) | | Clinical T stage, n (%) | | T1 | 16 (21.62) | 2 (2.70) | <0.01 | | T2 | 28 (37.84) | 42 (56.76) | | T3 | 20 (27.03) | 26 (35.14) | | T4 | 10 (13.51) | 4 (5.41) | | N stage, n (%) | | N0 | 70 (94.59) | 69 (93.24) | 0.73 | | N1 | 4 (5.41) | 5 (6.76) | | M stage, n (%) | | M0 | 72 (97.30) | 73 (98.65) | 0.56 | | M1 | 2 (2.70) | 1 (1.35) | | Biopsy Gleason grade group, n (%) | | I | 1 (1.35) | 0 (0.00) | <0.01 | | II | 7 (9.46) | 16 (21.62) | | III | 54 (72.97) | 56 (75.68) | | Unknown | 12 (16.22) | 2 (2.70) | | Biopsy Gleason score | | 6 | 8 (10.81) | 7 (9.46) | 0.90 | | 7 | 6 (8.11) | 7 (9.46) | | 8 | 14 (18.92) | 11 (14.86) | | Unknown | 46 (62.16) | 49 (66.22) |
|
|
Baseline characteristics of patients with DAC after propensity score matching.
|
| CSM | OM | | HR (95% CI) | p-Value | HR (95% CI) | p-Value | | RT | 1 | | 1 | | | RP vs. RT | 0.18 (0.04, 0.82) | 0.03 | 0.28 (0.11, 0.70) | 0.01 |
|
|
Cox proportional hazards regression models of CSM and OM after propensity score matching.
|
| [1] |
Global Burden of Disease Cancer Collaboration, Fitzmaurice C, Allen C, Barber RM, Barregard L, Bhutta ZA, et al. Global,regional, and national cancer incidence, mortality, years of life lost, years lived with disability, and disability-adjusted life-years for 32 cancer groups, 1990 to 2015: a systematic analysis for the global burden of disease study. JAMA Oncol 2017; 3:524e48.
|
| [2] |
Siegel RL, Miller KD, Jemal A. Cancer statistics, 2018. CA Cancer J Clin 2018; 68:7e30.
|
| [3] |
Melicow MM, Pachter MR. Endometrial carcinoma of prostatic utricle (uterus masculinus). Cancer 1967; 20:1715e22.
|
| [4] |
Marcus DM, Goodman M, Jani AB, Osunkoya AO, Rossi PJ. A comprehensive review of incidence and survival in patients with rare histological variants of prostate cancer in the United States from 1973 to 2008. Prostate Cancer Prostatic Dis 2012; 15:283e8.
|
| [5] |
Humphrey PA, Moch H, Cubilla AL, Ulbright TM, Reuter VE. The 2016 WHO classification of tumours of the urinary system and male genital organsdPart B: prostate and bladder tumours. Eur Urol 2016; 70:106e19.
|
| [6] |
Mottet N, Bellmunt J, Bolla M, Briers E, Cumberbatch MG, De Santis M, et al. EAU-ESTRO-SIOG guidelines on prostate cancer.Part 1: screening, diagnosis, and local treatment with curative intent. Eur Urol 2017; 71:618e29.
|
| [7] |
Meeks JJ, Zhao LC, Cashy J, Kundu S. Incidence and outcomes of ductal carcinoma of the prostate in the USA: analysis of data from the Surveillance, Epidemiology, and End Results program. BJU Int 2012; 109:831e4.
|
| [8] |
Wu YP, Chen SH, Wang ST, Li XD, Hai C, Lin YZ, et al. Prognostic values of clinicopathological characteristics and survival outcomes in prostate infiltrating ductal carcinoma: a population-based study. Oncotarget 2017; 8:29048e55.
|
| [9] |
Knipper S, Preisser F, Mazzone E, Mistretta FA, Tian Z, Briganti A, et al. Contemporary comparison of clinicopathologic characteristics and survival outcomes of prostate ductal carcinoma and acinar adenocarcinoma: a population-based study. Clin Genitourin Canc 2019; 17:231e7.
|
| [10] |
Packiam VT, Patel SG, Pariser JJ, Richards KA, Weiner AB, Paner GP, et al. Contemporary population-based comparison of localized ductal adenocarcinoma and high-risk acinar adenocarcinoma of the prostate. Urology 2015; 86:777e82.
|
| [11] |
Seipel AH, Delahunt B, Samaratunga H, Egevad L. Ductal adenocarcinoma of the prostate: histogenesis, biology and clinicopathological features. Pathology 2016; 48:398e405.
|
| [12] |
Epstein JI, Allsbrook Jr WC, Amin MB, Egevad LL, ISUP Grading Committee. The 2005 International Society of Urological Pathology (ISUP) consensus conference on Gleason grading of prostatic carcinoma. Am J Surg Pathol 2005; 29:1228e42.
|
| [13] |
Jeong SU, Kekatpure AK, Park JM, Han M, Hwang HS, Jeong HJ, et al. Diverse immunoprofile of ductal adenocarcinoma of the prostate with an emphasis on the prognostic factors. J Pathol Transl Med 2017; 51:471e81.
|
| [14] |
Gillard M, Lack J, Pontier A, Gandla D, Hatcher D, Adam GS, et al. Integrative genomic analysis of coincident cancer foci implicates CTNNB1 and PTEN alterations in ductal prostate cancer. Eur Urol Focus 2019; 5:433e42.
|
| [15] |
Bergamin S, Eade T, Kneebone A, Kench JG, Sved P, Biset JF, et al. Ductal carcinoma of the prostate: an uncommon entity with atypical behaviour. Clin Oncol 2019; 31:108e14.
|
| [16] |
Sha JJ, Bo J, Pan JJ, Zhang LH, Xuan HQ, Chen W, et al. Ductal adenocarcinoma of the prostate: immunohistochemical findings and clinical significance. Onco Targets Ther 2013; 6:1501e6.
|
| [17] |
Kan RW, Kan CF, Wong JH, Fu KK, Ng CF, Chan SW. Ductal adenocarcinoma of the prostate: a Hong Kong case series. Int Urol Nephrol 2014; 46:2133e7.
|
| [18] |
Tu SM, Lopez A, Leibovici D, Bilen MA, Evliyaoglu F, Aparicio A, et al. Ductal adenocarcinoma of the prostate: clinical features and implications after local therapy. Cancer 2009; 115:2872e80.
|
| [19] |
Orihuela E, Green JM. Ductal prostate cancer: contemporary management and outcomes. Urol Oncol 2008; 26:368e71.
|
| [20] |
I_gdem S, Spiegel DY, Efstathiou J, Miller RC, Poortmans PM, Koca S, et al. Prostatic duct adenocarcinoma: clinical characteristics,treatment options, and outcomesda Rare Cancer Network study. Onkologie 2010; 33:169e73.
|
| [21] |
Nakamura K, Terada N, Kobayashi T, Sugino Y, Yamasaki T, Matsui Y, et al. Clinical characteristics of prostate ductal adenocarcinoma in Kyoto University Hospital. Hinyokika Kiyo 2015; 61:487e91.
|
| [22] |
Greene FL, Page DL, Fleming ID, Fritz AG, Balch CM, Haller DG, et al. AJCC cancer staging manual. ed. 6. New York, NY: Springer Verlag; 2002. p. 301e47.
|
| [23] |
Edge S, Byrd DR, Compton CC, Fritz AG, Greene FL, Trotti A. AJCC cancer staging manual. ed. 7. New York, NY: Springer Verlag; 2009. p. 457e68.
|
| [24] |
Benedetto U, Head SJ, Angelini GD, Blackstone EH. Statistical primer: propensity score matching and its alternatives. Eur J Cardio Thorac Surg 2018; 53:1112e7.
|
| [25] |
Seipel AH, Wiklund F, Wiklund NP, Egevad L. Histopathological features of ductal adenocarcinoma of the prostate in 1,051 radical prostatectomy specimens. Virchows Arch 2013; 462:429e36.
|
| [26] |
Christensen WN, Steinberg G, Walsh PC, Epstein JI. Prostatic duct adenocarcinoma. Findings at radical prostatectomy. Cancer 1991; 67:2118e24.
|
| [27] |
Samaratunga H, Duffy D, Yaxley J, Delahunt B. Any proportion of ductal adenocarcinoma in radical prostatectomy specimens predicts extraprostatic extension. Hum Pathol 2010; 41:281e5.
|
| [28] |
Seipel AH, Delahunt B, Samaratunga H, Amin M, Barton J, Berney DM, et al. Diagnostic criteria for ductal adenocarcinoma of the prostate: interobserver variability among 20 expert uropathologists. Histopathology 2014; 65:216e27.
|
| [1] |
Fubo Wang,Chao Zhang,Fei Guo,Xia Sheng,Jin Ji,Yalong Xu,Zhi Cao,Ji Lyu,Xiaoying Lu,Bo Yang. The application of virtual reality training for anastomosis during robot-assisted radical prostatectomy[J]. Asian Journal of Urology, 2021, 8(2): 204-208. |
| [2] |
Anup Kumar,Vipul R. Patel,Sridhar Panaiyadiyan,Kulthe Ramesh Seetharam Bhat,Marcio Covas Moschovas,Brusabhanu Nayak. Nerve-sparing robot-assisted radical prostatectomy: Current perspectives[J]. Asian Journal of Urology, 2021, 8(1): 2-13. |
| [3] |
Anne Holck Storås,Martin G. Sanda,Olatz Garin,Peter Chang,Dattatraya Patil,Catrina Crociani,Jose Francisco Suarez,Milada Cvancarova,Jon Håvard Loge,Sophie D. Fosså. A prospective study of patient reported urinary incontinence among American, Norwegian and Spanish men 1 year after prostatectomy[J]. Asian Journal of Urology, 2020, 7(2): 161-169. |
| [4] |
Kerri Beckmann,Michael O’Callaghan,Andrew Vincent,Penelope Cohen,Martin Borg,David Roder,Sue Evans,Jeremy Millar,Kim Moretti. Extent and predictors of grade upgrading and downgrading in an Australian cohort according to the new prostate cancer grade groupings[J]. Asian Journal of Urology, 2019, 6(4): 321-329. |
| [5] |
Hendrik van Poppel , Wouter Everaerts , Lorenzo Tosco, Steven Joniau. Open and robotic radical prostatectomy[J]. Asian Journal of Urology, 2019, 6(2): 125-128. |
| [6] |
Michel Bolla , Ann Henry , Malcom Mason , Thomas Wiegel . The role of radiotherapy in localised and locally advanced prostate cancer[J]. Asian Journal of Urology, 2019, 6(2): 153-161. |
| [7] |
Najib Isse Dirie, Gaurab Pokhrel , Wei Guan, Mukhtar Adan Mumin, Jun Yang, Jackson Ferdinand Masau, Henglong Hu, Shaogang Wang. Is Retzius-sparing robot-assisted radical prostatectomy associated with better functional and oncological outcomes? Literature review and meta-analysis[J]. Asian Journal of Urology, 2019, 6(2): 174-182. |
| [8] |
Rei Umezawa, Koji Inaba, Satoshi Nakamura, Akihisa Wakita, Hiroyuki Okamoto, Keisuke Tsuchida, Tairo Kashihara, Kazuma Kobayashi, Ken Harada, Kana Takahashi, Naoya Murakami, Yoshinori Ito, Hiroshi Igaki, Keiichi Jingu, Jun Itami. Dose escalation of external beam radiotherapy for high-risk prostate cancer—Impact of multiple high-risk factor[J]. Asian Journal of Urology, 2019, 6(2): 192-199. |
| [9] |
Shulian Chen,Rang Gao,Hong Li,Kunjie Wang. Management of acquired rectourethral fistulas in adults[J]. Asian Journal of Urology, 2018, 5(3): 149-154. |
| [10] |
Chen Kenneth,Sim Allen,Kan Alex Ford. The effect of adjunct caudal block on postoperative analgesia in robot-assisted laparoscopic radical prostatectomy: A prospective randomized controlled, single blinded pilot study in a tertiary centre[J]. Asian Journal of Urology, 2018, 5(2): 122-126. |
| [11] |
Antonio B. Porcaro, Nicolò de Luyk, Paolo Corsi, Marco Sebben, Alessandro Tafuri, Davide Inverardi, Davide De Marchi, Irene Tamanini, Matteo Brunelli, Maria Angela Cerruto, Gian Luca Salvagno, Gian Cesare Guidi, Walter Artibani. Robotic assisted radical prostatectomy accelerates postoperative stress recovery: Final results of a contemporary prospective study assessing pathophysiology of cortisol peri-operative kinetics in prostate cancer surgery[J]. Asian Journal of Urology, 2016, 3(2): 88-95. |
| [12] |
Haifeng Wang, Xu Gao, Ziyu Fang, Xin Lu, Yan Wang, Chunfei Ma, Zhenkai Shi, Bo Yang, Shancheng Ren, Chuanliang Xu, Yinghao Sun. The older the better: The characteristic of localized prostate cancer in Chinese men[J]. Asian Journal of Urology, 2015, 2(3): 129-132. |
| [13] |
Deepansh Dalela, Rajesh Ahlawat, Akshay Sood, Wooju Jeong, Mahendra Bhandari, Mani Menon. The growth of computer-assisted (robotic) surgery in urology 2000-2014: The role of Asian surgeons[J]. Asian Journal of Urology, 2015, 2(1): 1-10. |
| [14] |
Zachary B. Koloff, Daniel A. Hamstra, John T. Wei, Jeffrey S. Montgomery, Scott A. Tomlins, Angela J. Wu, Todd M. Morgan, Javed Siddiqui, Kellie Paich, Arul M. Chinnaiyan, Felix Y. Feng, Alon Z. Weizer, Lakshmi P. Kunju, Brent K. Hollenbeck, David C. Miller, Ganesh S. Palapattu, Rohit Mehra. Impact of tertiary Gleason pattern 5 on prostate cancer aggressiveness: Lessons from a contemporary single institution radical prostatectomy series[J]. Asian Journal of Urology, 2015, 2(1): 53-58. |
| [15] |
Hendrik van Poppel. Locally advanced and high risk prostate cancer: the best indication for initial radical prostatectomy?[J]. Asian Journal of Urology, 2014, 1(1): 38-43. |
|
|
|
|