|
|
|
| Comparative study of on-demand and daily use of sertraline in treatment of premature ejaculation: A randomized clinical trial |
Soheila Siroosbakhta,Sadra Rezakhanihab,Bijan Rezakhanihac,*( ) )
|
a Faculty of Medicine, Imam Reza Hospital, Aja University of Medical Sciences, Tehran, Iran
b Department of Nutrition, Science and Research Islamic Azad University, Tehran, Iran
c Department of Urology, Imam Reza Hospital, Aja University of Medical Sciences, Tehran, Iran |
|
|
|
|
Abstract Objective The intravaginal ejaculatory latency time (IELT) may increase less in on-demand compared to daily intake, but may fulfill a suitable treatment for specific patients. We decided to compare the efficacy and safety of on-demand and daily use of sertraline in order to find the most effective and least complicated method in treatment of premature ejaculation (PE).
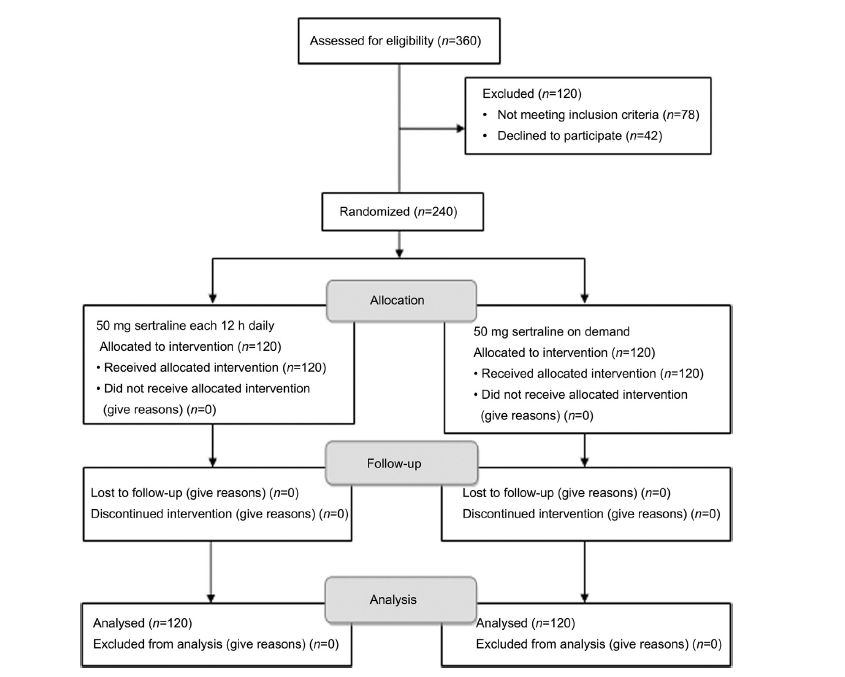
Methods This study was parallel or concurrent control randomized clinical trial. Two hundred and forty patients with PE diagnosed by urologist in the two groups of 120 from July 2017 to February 2019 enrolled in the study. In the first group, it is prescribed 50 mg sertraline each 12 h daily and the second group received 50 mg 4 h before coitus for 4 and 8 weeks. The IELT before treatment and during all coitus after treatment were recorded by the patient's wife with a stopwatch.
Results Mean IELT before, 4 and 8 weeks after treatment in two groups were: On-demand group 101.62±65.44 s, 208.75±128.02 s and 265.87±145.70 s; daily use group 102.50±81.22 s, 276.87±181.08 s and 353.75±176.45 s, respectively. The ejaculation time increased significantly in both groups (p<0.05). However, increase in ejaculation time in daily use group was significantly higher than the on-demand group in 4 weeks (p=0.036), especially in 8 weeks (p=0.009). The percent of side effects in daily use group (26.7%) was higher than on-demand group (20%) (p<0.05). Drowsiness, diarrhea and vertigo were significantly higher in the daily use than on-demand (p<0.05).
Conclusions On-demand and daily use of sertraline are effective and usually have no serious complications, but the on-demand method is considerably more tolerable. In patients who did not tolerate to daily use of this drug, on-demand could be used as a salvage therapy.
|
|
Received: 24 April 2019
Available online: 18 October 2019
|
|
Corresponding Authors:
Bijan Rezakhaniha
E-mail: reza.bijan@yahoo.com
|
|
|
|
|
Flow diagram of the study.
|

| Method | Group | Ejaculation time, mean | Number | p-Value | | On-demanda | Pair 1 | Before treatment, t=101.62 s
4 weeks later, t=208.75 | 120 | 0.000 | | Pair 2 | Before treatment, t=101.62 s
8 weeks later, t=265.87 s | 120 | 0.000 | | Pair 3 | 4 weeks later, t=208.75 s
8 weeks later, t=265.87 s | 120 | 0.000 | | Daily useb | Pair 1 | Before treatment, t=102.50 s
4 weeks later, t=276.87 s | 120 | 0.000 | | Pair 2 | Before treatment, t=102.50 s
8 weeks later, t=353.75 s | 120 | 0.000 | | Pair 3 | 4 weeks later, t=276.87 s
8 weeks later, t=353.75 s | 120 | 0.000 |
|
|
Statistical analysis of both methods of sertraline in treatment of premature ejaculation*.
|
| Ejaculation time | Groups | Number | Mean, s | Standard Deviation, s | p-Value | | Before treatment | On-demand | 120 | 101.62 | 65.44 | 0.954* | | Daily use | 120 | 102.50 | 81.22 | | | 4 weeks later | On-demand | 120 | 208.75 | 128.02 | 0.036? | | Daily use | 120 | 276.87 | 181.08 | | | 8 weeks later | On-demand | 120 | 265.87 | 145.70 | 0.009? | | Daily use | 120 | 353.75 | 176.45 | |
|
|
Comparison of ejaculation time before, 4 and 8 weeks after treatment in on-demand and daily use of sertraline.
|
| Side effects | On-demand | Each 12 h daily | p-Value | | Insomnia | 2 | 2 | 0.64 | | Drowsinessb | 6 | 10 | 0.04 | | Dyspepsia | 2 | 2 | 0.61 | | Diarrhea | - | 3 | 0.05 | | nausea | 2 | 2 | 0.61 | | Loss of appetite | 1 | 1 | 0.72 | | Fatigueb | 7 | 8 | 0.77 | | Headache | 1 | 1 | 0.72 | | Vertigo | 1 | 2 | 0.05 | | Anexity | 1 | 1 | 0.72 | | Urinary retention | - | - | - | | Loss of sexual desire | - | - | - |
|
|
Side effects in four groups.a
|
| [1] |
Symonds T, Roblin D, Hart K, Althof S. Howdoes premature ejaculation impact a man s life? J Sex Marital Ther 2003; 29:361e70.
|
| [2] |
Serefoglu EC, McMahon CG, Waldinger MD, Althof SE, Shindel A, Adaikan G , et al. An evidence-based unified definition of lifelong and acquired premature ejaculation: report of the second international society for sexual medicine ad hoc committee for the definition of premature ejaculation. J Sex Med 2014; 11:1423e41.
|
| [3] |
McMahon CG, Porst H. Oral agents for the treatment of premature ejaculation: review of efficacy and safety in the context of the recent International Society for Sexual Medicine criteria for lifelong premature ejaculation. J Sex Med 2011; 8:2707e25.
|
| [4] |
Zargooshi J. Premature ejaculation: bother and intravaginal ejaculatory latency time in Iran. J Sex Med 2009; 6:3478e89.
|
| [5] |
Waldinger MD. Emerging drugs for premature ejaculation. Expert Opin Emerg Drugs 2006; 11:99e109.
|
| [6] |
Lu J, Zhang X, Wang H, Qing Z, Qing Z, Han P, et al. Short- and long-range synergism disorders in lifelong premature ejaculation evaluated using the functional connectivity density and network property. Neuroimage Clin 2018; 21:607e15.
|
| [7] |
Kilinc MF, Aydogmus Y, Yildiz Y, Doluoglu OG . Impact of physical activity on patient self-reported outcomes of lifelong premature ejaculation patients: results of a prospective,randomised, sham-controlled trial. Andrologia 2018;50:e12799. https://doi.org/10.1111/and.12799.
|
| [8] |
Yildiz Y, Kilinc MF, Doluoglu OG. Is there any association between regular physical activity and ejaculation time? Urol J 2018; 15:285e9.
|
| [9] |
Kendirci M, Salem E, Hellstrom WJ. Dapoxetine, a novel selective serotonin transport inhibitor for the treatment of premature ejaculation. Ther Clin Risk Manag 2007; 3:277e89.
|
| [10] |
Safarinejad MR, Hosseini SY. Safety and efficacy of citalopram in the treatment of premature ejaculation: a double-blind placebo-controlled, fixed dose, randomized study. Int J Impot Res 2006; 18:164e9.
|
| [11] |
Hisasue S. The drug treatment of premature ejaculation. Transl Androl Urol 2016; 5:482e6.
|
| [12] |
Wang WF, Chang L, Minhas S, Ralph DJ. Selective serotonin reuptake inhibitors in the treatment of premature ejaculation. Chin Med J 2007; 120:1000e6.
|
| [13] |
Castiglione F, Albersen M, Hedlund P, Gratzke C, Salonia A, Giuliano F. Current pharmacological management of premature ejaculation: a systematic review and meta-analysis. Eur Urol 2016; 69:904e16.
|
| [14] |
Montejo AL, Montejo L, Baldwin DS. The impact of severe mental disorders and psychotropic medications on sexual health and its implications for clinical management. World Psychiatry 2018; 17:3e11.
|
| [15] |
Rezakhaniha B, Siroosbakhat S. Comparative study of therapeutic effects of two medicinal procedures of citalopram in premature ejaculation. Biosci Biotech Res Asia 2014; 11:953e8.
|
| [16] |
Rezakhaniha B, Sirosbakht S. Efficacy of selective serotonin reuptake inhibitor (SSRI) in patient with premature ejaculation. IJRM 2010; 8:55e9.
|
| [17] |
Gur S, Sikka SC. The characterization, current medications,and promising therapeutics targets for premature ejaculation. Andrology 2015; 3:424e42.
|
| [18] |
Dadfar MR, Baghinia MR. Salvage use of citalopram for treatment of fluoxetine-resistant premature ejaculation in recently married men. A prospective clinical trial. Urol J 2010; 7:40e4.
|
| [19] |
Rezakhaniha B, Khoshdel AR. Comparative study of therapeutic effects of two medicinal procedures of fluoxetine in premature ejaculation. JAUMS 2011; 8:299e304.
|
| [20] |
Abourehab MA, Ahmed OA, Balata GF, Almalki WH. Selfassembled biodegradable polymeric micelles to improve dapoxetine delivery across the blood-brain barrier. Int J Nanomed 2018; 13:3679e87.
|
| [21] |
Li J, Liu D, Wu J, Fan X, Dong Q. Dapoxetine for the treatment of premature ejaculation: a meta-analysis of randomized controlled trials with trial sequential analysis. Ann Saudi Med 2018; 38:366e75.
|
| [22] |
Waldinger MD, Schweitzer DH. Premature ejaculation and pharmaceutical company-based medicine: the dapoxetine case. J Sex Med 2008; 5:966e97.
|
| No related articles found! |
|
|
|
|