|
|
|
| Impact of surgical volume and resident involvement on patency rates after vasectomy reversal—A 14-year experience in an open access system |
Alexandria M. Hertza,*( ),Andrew W. Stammb,Mark I. Andersona,Karen C. Bakerc ),Andrew W. Stammb,Mark I. Andersona,Karen C. Bakerc
|
a Department of Urology, Madigan Army Medical Center, Tacoma, WA, USA
b Division of Urology and Transplantation, Virginia Mason Medical Center, Seattle, WA, USA
c Division of Urology, Duke University Hospital, Durham, NC, USA |
|
|
|
|
Abstract Objective Evaluate the influence of fellowship training, resident participation, reconstruction type, and patient factors on outcomes after vasectomy reversals in a high volume, open access system.
Methods Retrospective review of all vasectomy reversals performed at a single institution from January 1, 2002 to December 31, 2016 was conducted. Patient and spouse demographics, patient tobacco use and comorbidities, surgeon training and case volume, resident participation, reconstruction type, and postoperative patency were collected and analyzed.
Results Five hundred and twenty-six vasectomy reversals were performed during the study period. Follow-up was available in 80.6% of the cohort and overall patency, regardless of reconstruction type was 88.7%. The mean time to reversal was 7.87 years (range of 0-34 years). The majority of cases included resident participation. Case volume was high with faculty and residents logging a mean of 37.0 and 38.7 (median 18 and 37) cases respectively. Bilateral vasovasostomy was the most common reconstruction type (83%) and demonstrated a significantly better patency rate (89%) than all other reconstructions (p=0.0008). Overall patency and patency by reconstruction type were not statistically different among faculty surgeons and were not impacted by fertility fellowship training, resident participation or post-graduate year. Multivariate analysis demonstrated that increased time to reversal and repeat reconstructions had a negative impact on patency (p=0.0023 and p=0.043, respectively).
Conclusions Surgeons with a high volume of vasectomy reversals have outcomes consistent with contemporary series regardless of fellowship training in fertility. Patency was better for bilateral vasovasostomies. Patency was not negatively impacted by tobacco use, comorbidities, resident participation, or post-graduate year.
|
|
Received: 22 April 2019
Available online: 23 April 2020
|
|
Corresponding Authors:
Alexandria M. Hertz
E-mail: alexandria.m.hertz.mil@mail.mil
|
|
|

| Characteristics | Patients for all surgeons (n=526) | Patients for fellowship trained surgeons (n=120) | Patients for non-fellowship trained surgeons (n=406) | | Age at reconstruction, mean (range), year | 36.56 (23-76) | 36.94 (23-76) | 36.44 (23-64) | | Spouse age at reconstruction, mean (range), year | 31.01 (19-46) | 31.17 (19-42) | 30.95 (19-46) | | Time since reversal, mean (range), year | 7.87 (0-34) | 7.73 (0-34) | 7.92 (0-30) | | Post-graduate year of resident involved, mean (range), year | 3.65 (1-6) | 3.51 (1-6) | 3.70 (1-6) | | Active tobacco use at time of reconstruction, n (%) | 151 (28.7) | 76 (57.1)?? | 75 (19.1) | | Re-do reversal performed, n (%) | 34 (6.5) | 3 (2.5) | 31 (7.6)? | | Comorbidities (one or more), n (%) | 193 (36.7) | 76 (57.1)?? | 117 (29.7) | | Pain as an indication, n (%) | 9 (1.7) | 3 (2.5) | 6 (1.5) | | Postoperative semen analysis or report of pregnancy, n (%) | 423 (80.4) | 100 (83.3) | 323 (79.6) |
|
|
Characteristics of the surgical cohort broken down by fellowship status.
|
| Reconstruction type | Patency, % (number patent/total number) | p-Value | | All surgeons | Fellowship trained surgeons | Non-fellowship trained surgeons | | | All reconstructions | 87.0 (368/423) | 90 (100/111) | 85.9 (268/312) | 0.32 | | Reconstructions by subtype | | Bilateral vasovasostomy | 88.7 (315/355) | 90.7 (78/86) | 88.1 (237/269) | 0.56 | | Bilateral vasoepididymostomy | 54.6 (6/11) | 50 (3/6) | 60 (3/5) | 1.0 | | Unilateral vasovasostomy | 76.7 (23/30) | 100 (7/7) | 69.5 (16/23) | 0.15 | | Unilateral vasoepididymostomy | 60.0 (3/5) | 100 (2/2) | 33.3 (1/3) | 0.4 | | Vasovasostomy/Vasoepididymostomy | 95.5 (21/22) | 100 (10/10) | 91.67 (11/12) | 1.0 |
|
|
The surgical outcomes by reconstruction type and fellowship status.
|
| Patency | Attending surgeon A | Attending surgeon B | Attending surgeon C | | First 10 cases | Final 10 cases | First 10 cases | Final 10 cases | First 10 cases | Final 10 cases | | Patent/not patent | Patent | Patent | Patent | Patent | Patent | Patent | | Patent | Patent | Patent | Patent | Not patent | Patent | | Patent | Patent | Patent | Patent | Not patent | Patent | | Patent | Patent | Patent | Patent | Patent | Patent | | Patent | Patent | Patent | Patent | Patent | Not patent | | Not patent | Patent | Not patent | Patent | Patent | Not patent | | Patent | Patent | Patent | Patent | Not patent | Patent | | Patent | Patent | Patent | Patent | Patent | Patent | | Patent | Patent | Patent | Patent | Patent | Not patent | | Patent | Patent | Patent | Patent | Patent | Patent | | Patency rate (%) | 90 | 100 | 90 | 100 | 70 | 70 |
|
|
Patency of first 10 and last 10 reconstructions.
|
|
|
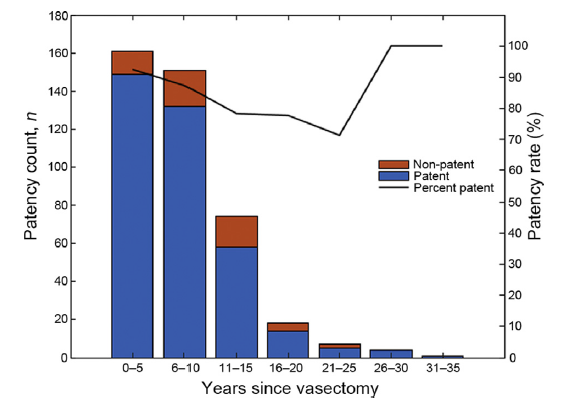
Number of reconstruction (all types) and postoperative patency rate categorized by years since vasectomy.
|
| Characteristics | p-Valuea | t or F-Value | 95% confidence interval | | Univariate factors | | Time to reversal | 0.0023 | t=3.173 | 0.91-3.99 | | Patient age | 0.093 | t=1.703 | -0.31 to 3.97 | | Tobacco use | 0.16 | t=-1.423 | -0.06 to 0.009 | | Medical comorbidities | 0.59 | t=-0.54 | -0.08 to 0.047 | | Resident PGY | 0.19 | t=1.34 | -0.16 to 0.81 | | Multivariate factors | | Reversal type-bilateral vasovasostomy | 0.0008 | F=5.469 | 1.77-2.05 | | Repeat reversal and category | 0.043 | F=2.587 | 0.006-0.360 | | Fellowship training and bilateral VV | 0.0686 | F=-1.825 | 2.481-3.198 | | Fellowship training and unilateral VV | 0.406 | F=-0.83 | 1.592-2.688 | | Fellowship training and unilateral VE | 0.604 | F=0.519 | 0.644-3.09 | | Fellowship training and VV/VE | 0.075 | F=-1.786 | 1.303-2.419 | | Fellowship training and bilateral VE | 1.0 | F=0.833 | 0.114-6.11 |
|
|
Factors affecting patency.
|
| [1] |
Eisenberg ML, Lipshultz LI. Estimating the number of vasectomies performed annually in the United States: data from the national survey of family growth. J Urol 2010; 184:2068e72.
|
| [2] |
Sandlow JI, Westefeld JS, Maples MR, Scheel KR. Psychological correlates of vasectomy. Fertil Steril 2001; 75:544e8.
|
| [3] |
Fox M. Vasectomy reversaldmicrosurgery for best results. Br J Urol 2018; 73:449e53.
|
| [4] |
Dewire DM, Lawson RK. Experience with macroscopic vasectomy reversal at the Medical College of Wisconsin. Wis Med J 2018; 93:107e9.
|
| [5] |
Jee SH, Hong YK. One-layer vasovasostomy: microsurgical versus loupe-assisted. Fertil Steril 2010; 94:2308e11.
|
| [6] |
Lee L, McLoughlin MG . Vasovasostomy: a comparison of macroscopic and microscopic techniques at one institution. Fertil Steril 1980; 33:54e5.
|
| [7] |
Bach PV, Patel N, Najari BB, Oromendia C, Flannigan R, Brannigan R, et al. Changes in practice patterns in male infertility cases in the United States: the trend toward subspecialization. Fertil Steril 2018; 110:76e82.
|
| [8] |
Nseyo U, Patel N, Hsieh TC. Vasectomy reversal surgical patterns:an analysis of the American Board of Urology Case Logs. Urology 2017; 107:107e13.
|
| [9] |
Ramasamy R, Mata DA, Jain L, Perkins AR, Marks SH, Lipshultz LI. Microscopic visualization of intravasal spermatozoa is positively associated with patency after bilateral microsurgical vasovasostomy. Andrology 2015; 3:532e5.
|
| [10] |
Herrel LA, Goodman M, Goldstein M, Hsiao W. Outcomes of microsurgical vasovasostomy for vasectomy reversal: a meta-analysis and systematic review. Urology 2015; 85:819e25.
|
| [11] |
Elzanaty S, Dohle GR. Vasovasostomy and predictors of vasal patency: a systematic review. Scand J Urol Nephrol 2012; 46:241e6.
|
| [12] |
Bolduc S, Fischer MA, Deceuninck G, Thabet M. Factors predicting overall success: a review of 747 microsurgical vasovasostomies. Can Urol Assoc J 2007; 1:388e94.
|
| [13] |
Ostrowski KA, Polackwich AS, Kent J, Conlin MJ, Hedges JC, Fuchs EF. Higher outcomes of vasectomy reversal in men with the same female partner as before vasectomy. J Urol 2015; 193:245e7.
|
| [14] |
Cosentino M, Peraza MF, Vives A, Sanchez J, Moreno D, Perona J, et al. Factors predicting success after microsurgical vasovasostomy. Int Urol Nephrol 2018; 50:625e32.
|
| [15] |
Patel V, Tully A, Holmes R, Lindsay J. Robotic radical prostatectomy in the community settingdthe learning curve and beyond: initial 200 cases. J Urol 2005; 174:269e72.
|
| [16] |
S?rensen LT, J?rgensen T, Kirkeby LT, Skovdal J, Vennits B, Wille-J?rgensen P. Smoking and alcohol abuse are major risk factors for anastomotic leakage in colorectal surgery. Br J Surg 1999; 86:927e31.
|
| [17] |
Tosun Z, Karabekmez FE, Duymaz A, ?zkan A, Keskin M, Avunduk MC. Preventing negative effects of smoking on microarterial anastomosis. Ann Plast Surg 2010; 65:91e5.
|
| [18] |
Hollingsworth MR, Sandlow JI, Schrepferman CG, Brannigan RE, Kolettis PN. Repeat vasectomy reversal yields high success rates. Fertil Steril 2007; 88:217e9.
|
| [19] |
Hernandez J, Sabanegh ES. Repeat vasectomy reversal after initial failure: overall results and predictors for success. J Urol 1999; 161:1153e6.
|
| [20] |
Fuchs EF, Burt RA. Vasectomy reversal performed15 years or more after vasectomy: correlation of pregnancy outcome with partner age and with pregnancy results of in vitro fertilization with intracytoplasmic sperm injection. Fertil Steril 2018; 77:516e9.
|
| [21] |
Holman CD, Wisniewski ZS, Semmens JB, Rouse IL, Bass AJ. Population-based outcomes after 28 246 in-hospital vasectomies and 1902 vasovasostomies in Western Australia. BJU Int 2000; 86:1043e9.
|
| [22] |
van Dongen J, Tekle FB, van Roijen JH. Pregnancy rate after vasectomy reversal in a contemporary series: influence of smoking, semen quality and post-surgical use of assisted reproductive techniques. BJU Int 2012; 110:562e7.
|
| [1] |
Huan Chen, Bijun Lian, Zhenyang Dong, Yan Wang, Min Qu, Feng Zhu, Yinghao Sun, Xu Gao. Experience of one single surgeon with the first 500 robot-assisted laparoscopic prostatectomy cases in mainland China[J]. Asian Journal of Urology, 2020, 7(2): 170-176. |
| [2] |
Kirsten JC Janosek-Albright, Peter N. Schlegel, Ali A. Dabaja. Testis sperm extraction[J]. Asian Journal of Urology, 2015, 2(2): 79-84. |
| [3] |
Bruno Camargo Tiseo, Russell Paul Hayden, Cigdem Tanrikut. Surgical management of nonobstructive azoospermia[J]. Asian Journal of Urology, 2015, 2(2): 85-91. |
|
|
|
|