|
|
|
| Treatment of clinical stage I non-seminoma |
Christian Winter( ),Andreas Hiester ),Andreas Hiester
|
| Department of Urology, University of Duesseldorf, Medical Faculty, Heinrich-Heine-University,Duesseldorf, Germany |
|
|
|
|
Abstract Germ cell cancers are the most common solid tumors among men between 15 and 40 years. Non-seminomatous germ cell tumors (NSGCTs) represent a unique and exclusive cohort of germ cell tumor patients. Non-seminoma can harbor different histologic components. The most commonly found histologies are embryonal cell cancer, teratoma, yolk sack tumor and choriocarcinoma, as well as teratocarcinoma and seminoma, in combination with non-seminomatous germ cell tumors histologic types. The clinical definition of stage I non-seminoma is the absence of metastatic lesions on imaging and normal tumor markers. The cure rate for clinical stage I NSGCT is 99% and this can be achieved by three therapeutic strategies: Active surveillance with treatment at the time of relapse, retroperitoneal lymph node dissection or adjuvant chemotherapy. The balancing of these various strategies should always be based on an individual risk profile of NGSCG patient depending on the lymphovascular invasion of the tumor.
|
|
Received: 07 November 2019
Available online: 06 March 2021
|
|
Corresponding Authors:
Christian Winter
E-mail: christian.winter@med.uni-duesseldorf.de
|
|
|
|
|
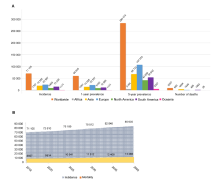
The worldwide incidence for testis cancer Incidence. (A) 1-year and 5-year prevalence and number of deaths in 2018 for testicular cancer; (B) Expected number of incident cases and deaths from 2018 to 2040 for testicular cancer. (GLOBOCAN 2018, https://gco.iarc.fr/).
|

| Clinical stage | Characteristic | | Stage 0 | pTis | N0 | M0 | S0, SX | | Stage I | pT1-pT4 | N0 | M0 | SX | | Stage IA | pT1 | N0 | M0 | S0 | | Stage IB | pT2-pT4 | N0 | M0 | S0 | | Stage IS | Any pT | N0 | M0 | S1-3 |
|
|
Stage grouping for NSGCT (up to Stage I) [5].
|
|
|
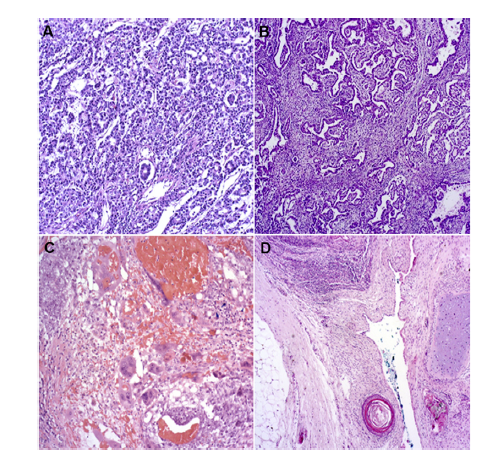
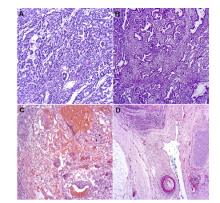
The results of histochemical staining. (A) Microscope slides of yolk sac (10×); (B) embryonal cell carcinoma (5×); (C) choriocarcinoma (10×); (D) teratoma (5×).
|
| Dose-related | Non-dose related | Unknown | | Infertility | Febrile neutropenia | Second malignancy | | Peripheral neuropathy | Alopecia | Cardiovascular disease | | Ototoxicity | Nausea/vomiting | - | | Raynaud's phenomena | - | - | | Fatigue | - | - | | Skin toxicity | - | - | | Avascular necrosis hip | - | - | | Pneumonitis/Lung fibrosis | - | - | | Renal damage | - | - | | Anaemia | - | - | | Metabolic syndrome | - | - |
|
|
Dose-related and non-dose related toxicities of BEP chemotherapy [58].
|
| Complication | Percent (%) | | Retrograde ejaculation | 6.7 | | Wound infection | 5.4 | | Ileus | 2.1 | | Chylous ascites | 2.1 | | Vascular lesion with intraoperative repair | 2.0 | | Lymphocele | 1.7 | | Hydronephrosis | 1.2 | | Ventral hernia | 0.8 | | Stomach ulcer | 0.8 | | Lung embolism | 0.8 | | Keloid | 0.8 | | Bleeding | 0.8 | | Urinary tract infection | 0.4 | | Ureteral lesion with ureteral stent insertion | 0.4 | | Small bowel obstruction | 0.4 | | Renal artery lesion with Nephrectomy | 0.4 | | Pneumonia | 0.4 | | Large bowel lesion with intraoperative repair | 0.4 | | Inferior mesenteric artery lesion with hemicolectomy and temporary colostomy | 0.4 | | Epididymitis | 0.4 | | Deep vein thrombosis | 0.4 |
|
|
Intraoperative, early and late complications of retroperitoneal lymph node dissection [47].
|
| NCCN guidelines | Year 1 | Year 2 | Year 3 | Year 4 | Year 5 | | Physical examination | Every 2 months | Every 3 months | Every 4-6 months | Every 6 months | Annually | | Tumor marker | Every 2 months | Every 3 months | Every 4-6 months | Every 6 months | annually | | Chest X-ray | 2 times (at month 4 and 12) | Annually | Annually | Annually | Annually | | Abdominopelvic CT scan | 2-3 times | Annually | Annually | No scan | No scan |
|
|
Follow-up clinical stage I NSGCT without risk factors according to the NCCN guidelines [22].
|
| NCCN guideline | Year 1 | Year 2 | Year 3 | Year 4 | Year 5 | | Physical examination | Every 2 months | Every 3 months | Every 4-6 months | Every 6 months | Annually | | Tumor marker | Every 2 months | Every 3 months | Every 4-6 months | Every 6 months | Annually | | Chest X-ray | Every 4 months | Every 4-6 months | Every 6 months | Annually | Annually | | Abdominopelvic CT scan | Every 4 months | Every 4-6 months | Every 6 months | Annually | Annually |
|
|
Follow-up clinical stage I NSGCT with risk factors according to the NCCN guidelines [22].
|
|
|
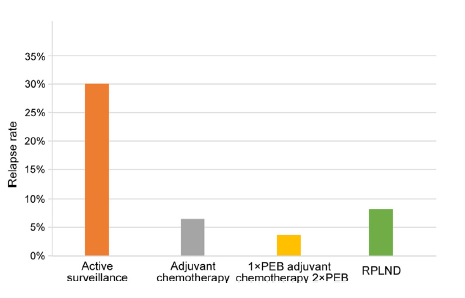
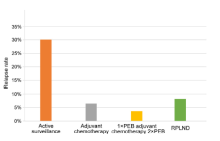
Relapse rates according to different treatment strategies for NSGCT stage I [39,40]. RPLND, retroperitoneal lymph node dissection; NSGCT, non-seminomatous germ cell tumors; BEP, bleomycin, etoposide, and cisplatin.
|

|
|
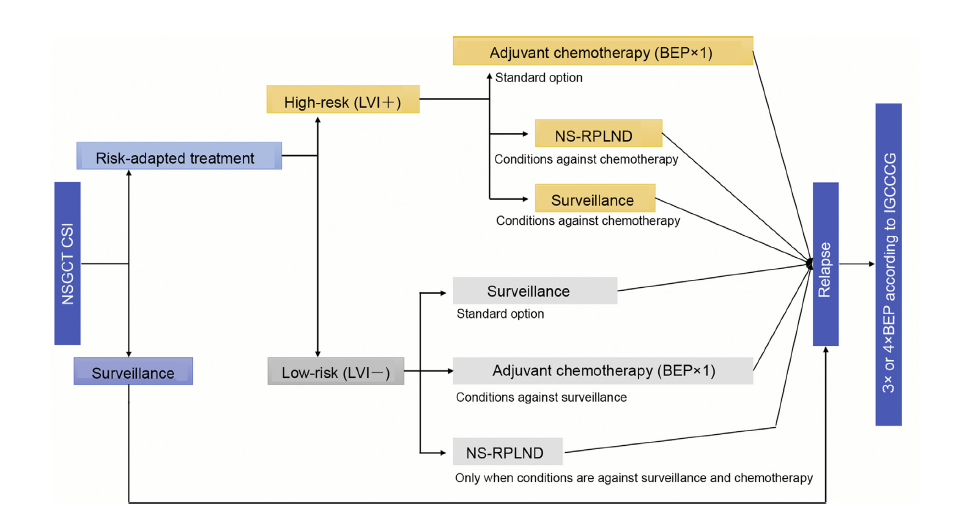
Flowsheet of treatment of NSGCT stage I (modified after [4]). NSGCT, non-seminomatous germ cell tumors; LVI+, lymphovascular invasion; LVI-, no lymphovascular invasion; IGCCCG, International Germ Cell Cancer Collaborative Group; BEP, bleomycin, etoposide, and cisplatin; NS-RPLND, nerve-sparing retroperitoneal lymph node dissection; NSGCT, non-seminomatous germ cell tumor; CSI, clinical stage I.
|
| [1] |
Shanmugalingam T, Soultati A, Chowdhury S, Rudman S, Van Hemelrijck M. Global incidence and outcome of testicular cancer. Clin Epidemiol 2013; 5:417e27.
|
| [2] |
Le Cornet C, Lortet-Tieulent J, Forman D, Béranger R, Flechon A, Fervers B, et al. Testicular cancer incidence to rise by 25% by 2025 in Europe? Model-based predictions in 40countries using population-based registry data. Eur J Canc 2014; 50:831e9.
|
| [3] |
Ghazarian AA, Trabert B, Devesa SS, McGlynn KA. Recent trends in the incidence of testicular germ cell tumors in the United States. Andrology 2015; 3:13e8.
|
| [4] |
Albers P, Albrecht W, Algaba F, Bokemeyer C, Cohn-Cedermark G, Fizazi K, et al. Guidelines on testicular cancer:2015 update. Eur Urol 2015; 68:1054e68.
|
| [5] |
Wittekind C. [TNM classification of testicular tumors. Definitions and prerequisites for correct application]. Pathologe 2014; 35:252e5.
|
| [6] |
Winter C, Albers P. Testicular germ cell tumors: pathogenesis,diagnosis and treatment. Nat Rev Endocrinol 2011; 7:43e53.
|
| [7] |
Kollmannsberger C, Moore C, Chi KN, Murray N, Daneshmand S, Gleave M, et al. Non-risk-adapted surveillance for patients with stage I nonseminomatous testicular germcell tumors: diminishing treatment-related morbidity while maintaining efficacy. Ann Oncol 2010; 21:1296e301.
|
| [8] |
Kollmannsberger C, Tandstad T, Bedard PL, Cohn-Cedermark G, Chung PW, Jewett MA, et al. Patterns of relapse in patients with clinical stage I testicular cancer managed with active surveillance. J Clin Oncol 2015; 33:51e7.
|
| [9] |
Sturgeon JF, Moore MJ, Kakiashvili DM, Duran I, Anson-Cartwright LC, Berthold DR, et al. Non-risk-adapted surveillance in clinical stage I nonseminomatous germ cell tumors:the Princess Margaret Hospital’s experience. Eur Urol 2011; 59:556e62.
|
| [10] |
Daugaard G, Gundgaard MG, Mortensen MS, Agerb?k M, Holm NV, R?rth M, et al. Surveillance for stage I nonseminoma testicular cancer: outcomes and long-term follow-up in a population-based cohort. J Clin Oncol 2014; 32:3817e23.
|
| [11] |
Collette L, Sylvester RJ, Stenning SP, Fossa SD, Mead GM, de Wit R, et al. Impact of the treating institution on survival of patients with “poor-prognosis” metastatic nonseminoma. European Organization for Research and Treatment of Cancer GenitoeUrinary Tract Cancer Collaborative Group and the Medical Research Council Testicular Cancer Working Party. J Natl Cancer Inst 1999; 91:839e46.
|
| [12] |
Nayan M, Jewett MA, Anson-Cartwright L, Bedard PL, Moore M, Chung P, et al. The association between institution at orchiectomy and outcomes on active surveillance for clinical stage I germ cell tumours. Can Urol Assoc J 2016; 10:204e9.
|
| [13] |
Adra N, Althouse SK, Liu H, Brames MJ, Hanna NH, Einhorn LH, et al. Prognostic factors in patients with poor-risk germ-cell tumors: a retrospective analysis of the Indiana University experience from 1990 to 2014. Ann Oncol 2016; 27:875e9.
|
| [14] |
Stephenson A, Eggener SE, Bass EB, Chelnick DM, Daneshmand S, Feldman D, et al. Diagnosis and treatment of early stage testicular cancer: AUA guideline. J Urol 2019; 202:272e81.
|
| [15] |
Davis BE, Herr HW, Fair WR, Bosl GJ. The management of patients with nonseminomatous germ cell tumors of the testis with serologic disease only after orchiectomy. J Urol 1994; 152:111e4.
|
| [16] |
Capocaccia R, Gatta G, Dal Maso L. Life expectancy of colon,breast, and testicular cancer patients: an analysis of US-SEER population-based data. Ann Oncol 2015; 26:1263e8.
|
| [17] |
Albers P, Ulbright TM, Albers J, Miller GA, Orazi A, Crabtree WN, et al. Tumor proliferative activity is predictive of pathological stage in clinical stage A nonseminomatous testicular germ cell tumors. J Urol 1996; 155:579e86.
|
| [18] |
Albers P, Siener R, Kliesch S, Weissbach L, Krege S, Sparwasser C, et al. Risk factors for relapse in clinical stage I nonseminomatous testicular germ cell tumors: results of the German Testicular Cancer Study Group Trial. J Clin Oncol 2003; 21:1505e12.
|
| [19] |
Heidenreich A, Schenkmann NS, Sesterhenn IA, Mostofi FK, McCarthy WF, Heidenreich B, et al. Immunohistochemical expression of Ki-67 to predict lymph node involvement in clinical stage I nonseminomatous germ cell tumors. J Urol 1997; 158:620e5.
|
| [20] |
Nicolai N, Tarabelloni N, Gasperoni F, Catanzaro M, Stagni S, Torelli T, et al. Laparoscopic retroperitoneal lymph node dissection for clinical stage I nonseminomatous germ cell tumors of the testis: safety and efficacy analyses at a high volume center. J Urol 2018; 199:741e7.
|
| [21] |
Ondrus D, Matoska J, Belan V, Kausitz J, Goncalves F, Hornak M. Prognostic factors in clinical stage I nonseminomatous germ cell testicular tumors: rationale for different risk-adapted treatment. Eur Urol 1998; 33:562e6.
|
| [22] |
Motzer RJ, Jonasch E, Agarwal N, Beard C, Bhayani S, Bolger GB, et al. Testicular cancer, version 2.2015. J Natl Compr Canc Netw 2015; 13:772e99.
|
| [23] |
Leitlinienprogramm Onkologie (Deutsche Krebsgesellschaft,Deutsche Krebshilfe, AWMF): S3-Leitlinie Diagnostik, Therapie und Nachsorge der Keimzelltumoren des Hodens, Langversion 0.1 (Konsultationsfassung), 2018 AWMF Registernummer:043/049OL. https://www.leitlinienprogramm-onkologie.de/leitlinien/hodentumoren. [Accessed 18 April 2019].
|
| [24] |
Dieckmann KP, Radtke A, Geczi L, Matthies C, Anheuser P, Eckardt U, et al. Serum levels of microRNA-371a-3p (M371 test)as a new biomarker of testicular germ cell tumors: results of a prospective multicentric study. J Clin Oncol 2019; 37:1412e23.
|
| [25] |
Donadio AC, Motzer RJ, Bajorin DF, Kantoff PW, Sheinfeld J, Houldsworth J, et al. Chemotherapy for teratoma with malignant transformation. J Clin Oncol 2003; 21:4285e91.
|
| [26] |
El Mesbahi O, Terrier-Lacombe MJ, Rebischung C, Theodore C, Vanel D, Fizazi K. Chemotherapy in patients with teratoma with malignant transformation. Eur Urol 2007; 51:1306e12.
|
| [1] |
Zoe Loh,Todd G. Manning,Jonathan S. O’Brien,Marlon Perera,Nathan Lawrentschuk. Mesenteric metastases from mature teratoma of the testis: A case report[J]. Asian Journal of Urology, 2020, 7(3): 322-325. |
| [2] |
Olivier Rouviere , Paul Cezar Moldovan. The current role of prostate multiparametric magnetic resonance imaging[J]. Asian Journal of Urology, 2019, 6(2): 137-145. |
| [3] |
Laurence Klotz. Contemporary approach to active surveillance for favorable risk prostate cancer[J]. Asian Journal of Urology, 2019, 6(2): 146-152. |
| [4] |
Kenneth Chen,Kae Jack Tay,Yan Mee Law,Hakan Aydin,Henry Ho,Christopher Cheng,John Shyi Peng Yuen. Outcomes of combination MRI-targeted and transperineal template biopsy in restaging low-risk prostate cancer for active surveillance[J]. Asian Journal of Urology, 2018, 5(3): 184-193. |
|
|
|
|