|
|
|
| Totally intracorporeal robot-assisted urinary diversion for bladder cancer (part 2). Review and detailed characterization of the existing intracorporeal orthotopic ileal neobladder |
Hugo Otaola-Arcaa,b,Kulthe Ramesh Seetharam Bhatc,Vipul R. Patelc,Marcio Covas Moschovasc,Marcelo Orvietob,*( ) )
|
a Department of Urology, Clínica Alemana, Santiago, Chile
b School of Medicine, Clínica Alemana-Universidad del Desarrollo, Santiago, Chile
c Department of Robotic Surgery, AdventHealth Global Robotics Institute, Celebration, FL, USA |
|
|
|
|
Abstract Objective: To review the most used intracorporeal orthotopic ileal neobladder (ICONB) after radical cystectomy for bladder cancer and create a unified compendium of the different alternatives, including new consistent images. Methods: We performed a non-systematic review of the literature with the keywords “bladder cancer”, “urinary diversion”, “radical cystectomy”, and “neobladder”. Results: Forty studies were included in the analysis. The most frequent type of ICONB was the modified Studer “U” neobladder (70%) followed by the Hautmann “W” modified neobladder (7.5%), the “Y” neobladder (5%), and the Padua neobladder (5%). The operative time to perform a urinary diversion ranged from 124 to 553 min. The total estimated blood loss ranged from 200 to 900 mL. The rate of positive surgical margins ranged from 0% to 8.1%. Early minor and major complication rates ranged from 0% to 100% and from 0% to 33%, respectively. Late minor and major complication rates ranged from 0% to 70% and from 0% to 25%, respectively. Conclusion: The most frequent types of ICONB are Studer “U” neobladder, Hautmann “W” neobladder, “Y” neobladder, and the Padua neobladder. Randomized studies comparing the performance of the different types of ICONB, the performance in an intra or extracorporeal manner, or the performance of an ICONB versus ICIC are lacking in the literature. To this day, there are not sufficient quality data to determine the supremacy of one technique. This manuscript represents a compendium of the most used ICONB with detailed descriptions of the technical aspects, operative and perioperative outcomes, and new consistent images of each technique.
|
|
Received: 24 December 2019
Available online: 20 January 2021
|
|
Corresponding Authors:
Marcelo Orvieto
E-mail: morvieto@alemana.cl
|
|
|

| Study characteristics | Baseline and operative data | Complications | Continence at 12 months | | Study | Number of patients | Type of ICUD | Age (year) | Males (%) | Total OT (min) | ICUD OT (min) | EBL (mL) | PSM (%) | F-UP (month) | Early (<30 days) | Late (31-90 days) | Daytime (%) | Nighttime (%) | Potency (%) | | Clavien <III | Clavien ≥III | Clavien <III | Clavien ≥III | | Beecken et al. (2003) [13],a | 1 | Hautmann “W” | 58d | 100.0 | 510d | NA | 200d | 0.0 | 5.0d | 0.0 | 0.0 | 0.0 | 0.0 | NA | NA | NA | | Sala et al. (2006) [44],a | 1 | Hautmann “W” | 70d | 100.0 | 720d | 510d | 200d | 0.0 | 3.0d | 0.0 | 0.0 | NA | NA | 100.0g | 0.0g | NA | | Hussein et al. (2017) [45],a | 5 | Hautmann “W” | 57.0e | 80.0 | 357e | 193e | 225e | 0.0 | Min: 3 | 40.0 | 20.0 | 0.0 | 0.0 | NA | NA | NA | | Pruthi et al. (2010) [14],b | 12 | IC (75%)
Studer “U” (25%) | 60e | 75.0 | 318e | NA | 221e | NA | Min: 3 | 41.6 | 0.0 | 16.6 | 0.0 | NA | NA | NA | | Romero-González et al. (2011) [15],a | 1 | Studer “U” | 79d | 100.0 | 420d | 240d | 500d | 0.0 | 7.0h | 0.0 | 0.0 | NA | NA | NA | NA | NA | | Jonsson et al. (2011) [[16], [17], [18]],c | 45 | IC (20%)
Studer “U” (80%) | 73f
60f | 55.0
91.6 | 460f
480f | NA | 350f
480f | 2.2 | 32.0f
24.0f | 11.1
19.4 | 33.3
8.3 | 11.1
16.6 | 22.2
13.8 | NA
97.0 | NA
83.0 | NA
93.7 | | Akbulut et al. (2011) [19],a | 12 | ONB Studer “U” | 60e | 100.0 | 600e | NA | 455e | 0.0 | 7.1e | 50.0 | 16.0 | 25.0 | 16.6 | 100.0 | 71.4 | 25.0 | | Schumacher et al. (2011) [20],a | 48 | IC (20%)
Studer “U” (80%) | 62f | 84.4 | 477f | NA | 550f | 2.2 | 24.0e | 17.7 | 22.2 | 13.3 | 17.8 | NA | NA | NA | | Goh et al. (2012) [21],c | 15 | IC (47%)
Studer “U” (53%) | 69f
63f | 100.0
75.0 | 450f
450f | NA | 200f
225f | 0.0
0.0 | 3.3f
3.0f | 71.4
62.5 | 0.0
25.0 | 14.2
0.0 | 0.0
12.5 | NA
75.0 | NA
NA | NA
NA | | Canda et al. (2012) [22],a | 27 | IC (7%)
Studer “U” (93%) | 61.4e | 92.5 | 594e | NA | 429e | 3.7 | 6.3e | 33.3 | 14.8 | 14.8 | 11.1 | 64.7 | 17.6 | NA | | Haddad et al. (2013) [23],a | 1 | Studer “U” | 73d | 100.0 | 368d | 180d | 900d | 0.0 | 3.0d | 100.0 | 0.0 | NA | NA | NA | NA | NA | | Collins et al. (2013) [24],a | 113 | IC (38%)
Studer “U” (62%) | 69.9e
59.8e | 74.4
88.5 | 292f
420f | NA | 200f
500f | 11.6
1.5 | 4.0f
30.0f | 32.5
12.8 | 53.4
31.4 | 0.0
14.2 | 23.2
21.4 | NA | NA | NA | | Tyritzis et al. (2013) [25],a | 70 | Studer “U” | 59.8e | 95.7 | 420f | NA | 500f | 1.4 | 30.3f | 17.0 | 31.4 | 12.8 | 18.6 | 73.8 | 61.5 | 51.6 | | Desai et al. (2014) [26],c | 37 | IC (51%)
Studer “U” (49%) | 75f
62f | 84.0
72.0 | 386f
387f | 92f
124f | 250f
200f | 10.0
0.0 | 16.0f
12.0f | 42.0
67.0 | 27.0
6.0 | 47.0
67.0 | 32.0
17.0 | NA | NA | NA | | Collins et al. (2014) [27],a | 80 | Studer “U” | 64.0e | NA | 420f | NA | 475f | 4.0 | 31.0e | 17.0 | 27.0 | 11.0 | 19.0 | 87.0 | 80.0 | 69.0 | | Abreu et al. (2014) [28],c | 103 | IC (55%)
Studer “U” (45%) | 72f
60.5f | 75.0
89.0 | 396f
462f | NA | 250f
200f | 7.0
0.0 | NA | 42.0
41.0 | 23.0
21.0 | NA | NA | NA | NA | NA | | Desai et al. (2014) [32],a | 132 | Studer “U” | 60e | 86.4 | 456e | NA | 430e | 0.8 | 25.1e | 31.8 | 15.2 | 14.4 | 12.9 | 84.0h | 84.0h | NA | | Butt et al. (2015) [29],a | 4 | Studer “U” | 61.8e | 100.0 | 522e | NA | 237e | 0.0 | 21.0e | 50.0 | 0.0 | 25.0 | 25.0 | 100.0 | 75.0 | NA | | Atmaca et al. (2015) [30],a | 32 | Studer “U” | 62.2e | 90.6 | 585f | NA | 412f | 6.3 | Min: 9 | 62.5 | 19.0 | 15.6 | 6.3 | 84.6 | 46.1 | NA | | Schwentner et al. (2015) [31],a | 62 | Studer “U” | 63.6e | 80.6 | 476e | 183e | 385e | 6.4 | 37.3e | 24.2 | 25.8 | NA | NA | 88.0 | 55.1 | 54.0 | | Sim et al. (2015) [38],a | 101 | IC (28%)
Studer “U” (72%) | 76.1e
62.1e | 89.3
78.0 | 350e
452e | 133e
178e | 347e
347e | 14.3
6.8 | 22.5e
32.4e | 21.4
28.7 | 14.2
27.3 | 0.0
1.3 | 7.1
15.0 | NA
89.2 | NA
67.6 | 100.0
48.0 | | Koupparis et al. (2015) [33],b | 102 | IC (11%)
Studer “U” (89%) | 68.2e | 69.6 | NA | NA | NA | NA | NA | Early and late Clavien <III: 23.0
Early and late Clavien ≥III: 9.0 | NA | NA | NA | | Nyame et al. (2016) [34],a | 3 | Studer “U” | 35.3e | 100.0 | 473e | NA | 266e | 0.0 | 28.1e | 66.6 | 0.0 | 0.0 | 0.0 | 100.0 | 100.0 | 100.0 | | Almassi et al. (2016) [35],a | 19 | Studer “U” | 55.0e | 94.7 | 486e | NA | 300f | NA | NA | Early and late Clavien <III: 36.8
Early and late Clavien ≥III: 5.2 | NA | NA | NA | | Satkunasivam et al. (2016) [36],b | 28 | Studer “U” | 63f | 100.0 | NA | NA | NA | NA | 9.4f | NA | NA | NA | NA | 41.6 | 37.5 | NA | | Koie et al. (2018) [37],a | 22 | Studer “U” | 65f | 95.5 | 430f | 553f | 300f | 0.0 | 33.4f | 31.8 | 0.0 | 0.0 | 4.5 | 93.4 | 93.4 | NA | | Porreca et al. (2018) [39],c | 24 | IC (46%)
Studer “U” (54%) | 68f | 91.7 | 370f
410f | 106f
172f | 390f
440f | 9.0
0.0 | 6.5f
6.0f | 9.0
15.3 | 0.0
7.6 | 0.0
30.7 | 0.0
7.6 | 84.0 | 69.0 | 45 | | Chow et al. (2018) [40],b | 26 | IC (81%)
Studer “U” (15%) | 70f | 80.0 | 362f | NA | 300f | 4.0 | NA | Early and late Clavien <III: 62.2
Early and late Clavien ≥III: 19.0 | NA | NA | NA | | Lenfant et al. (2018) [41],b | 74 | IC (47%)
Studer “U” (53%) | 65f | 81.1 | 320f | NA | 400f | 8.1 | 15.0f | 37.8 | 9.4 | 6.7 | 12.1 | NA | NA | NA | | Porreca et al. (2019) [42],a | 100 | URS (17%)
IC (32%)
Studer “U” (51%) | 69f | 90.0 | 410f | 60f
120f
180f | 200f | 3.0 | 14.0f | 25.0 | 9.0 | 9.0 | 10.0 | NA
NA
90.2 | NA
NA
70.6 | 31.0 | | Brassetti et al. (2019) [43],a | 113 | IC (43%)
Studer “U” or Padua (57%) | 69e | 82.0 | 382e | NA | NA | 8.0 | NA | Clavien ≥III: 20.0 | NA | NA | NA | | Kang et al. (2012) [50],b | 4 | IC (75%)
Camey (35%) | 69.5e | 75.0 | 510e
585e | NA | 400e
500e | 0.0
0.0 | Min: 3 | 25.0 | 0.0 | 0.0 | 0.0 | NA | NA | NA | | Tan et al. (2015) [51],a | 20 | Pyramid pouch | 57.2e | 95.0 | 330f | 150f | 330f | NA | 21.5f | 70.0 | 0.0 | 70.0 | 25.0 | 95.0h | 70.0h | NA | | Sim et al. (2015) [46],a | 1 | “Y”-pouch | 67d | 100.0 | 340d | NA | Minimald | NA | NA | 0.0 | 0.0 | 0.0 | 0.0 | NA | NA | NA | | Asimakopoulos et al. (2016) [47],a | 40 | “Y”-pouch | 57e | 100.0 | 315f | NA | 395f | 2.5 | 26.5f | 27.5 | 2.0 | 27.5 | 5.0 | 100.0 | 72.0 | 72.0 | | Simone et al. (2018) [48],a | 45 | Padua | 65f | 71.1 | 305f | NA | 210f | 0.0 | Min: 24 | 24.4 | 0.0 | 33.3 | 8.8 | 73.3 | 55.5 | NA | | Simone et al. (2018) [49],a | 64 | Padua | 62.5e | 78.1 | NA | NA | NA | 0.0 | Min: 24 | Early and late Clavien <III: 35.9
Early and late Clavien ≥III: 6.3 | NA | NA | NA | | Cacciamani et al. (2019) [52],a | 15 | ra-VIP | 60f | 93.0 | 390f | NA | 300f | 7.0 | 17.0f | 13.0 | 33.0 | 0.0 | 7.0 | 62.0 | 38.0 | NA | | Minervini et al. (2018) [53],a | 18 | FloRIN | 66f | 89.0 | 450f | NA | NA | NA | NA | 22.2 | 16.6 | NA | NA | 77.8 | 66.7 | NA | | Hussein et al. (2018) [54],b | 1 094 | IC (79%)
ONB (21%) | 67e | 71.0 | 357f | NA | 300f | 7.0 | 11.0f | Early and late Clavien <III: 39.0
Early and late Clavien ≥III: 11.0 | NA | NA | NA |
|
|
Study characteristics, baseline, operative data, and complications after robot-assisted intracorporeal orthotopic neobladder.
|
|
|
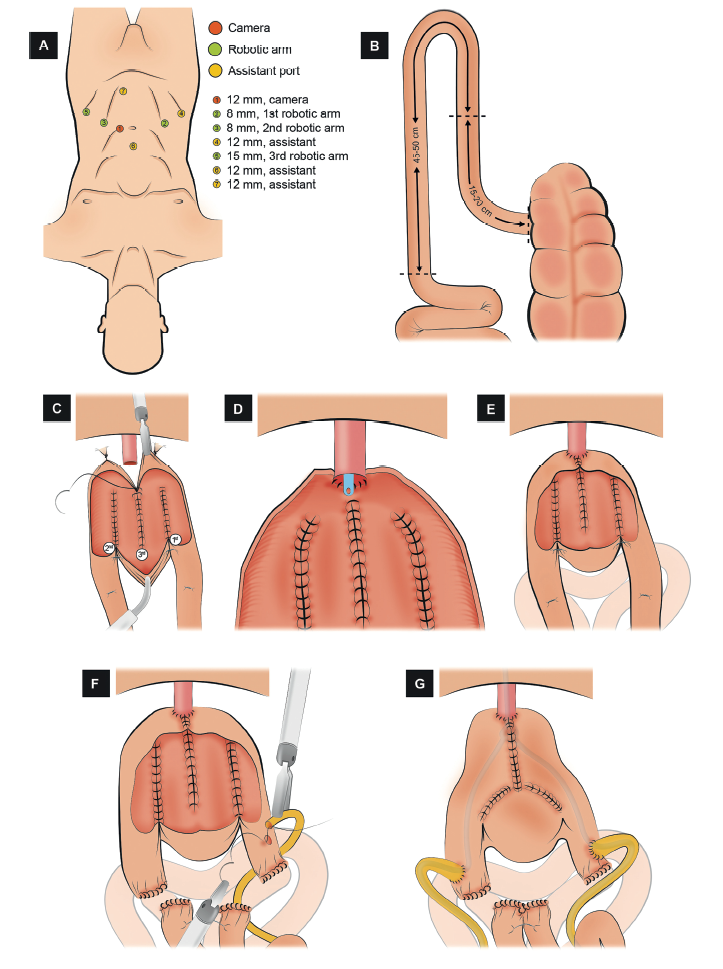
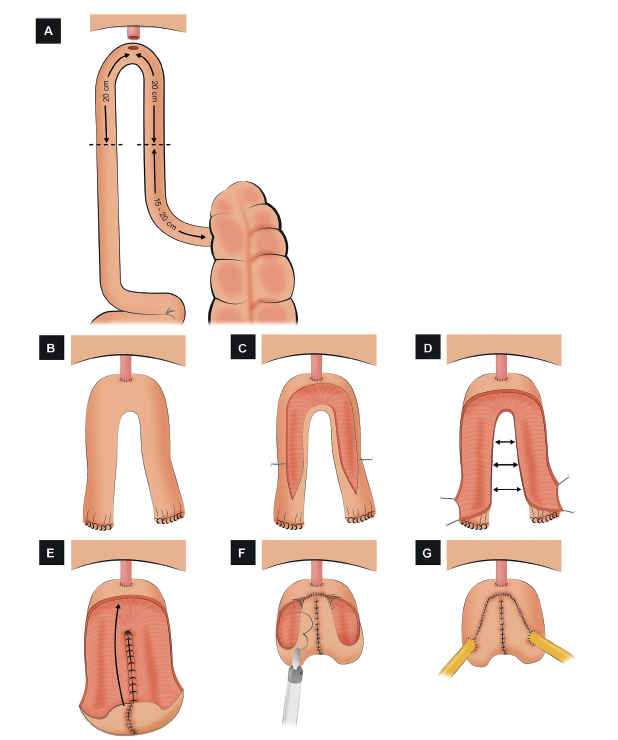
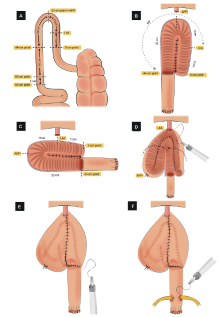
Schematic figure demonstrating the step-by-step creation of the robotic Hautmann “W” ICONB (Adapted from Hussein et al. [45]). (A) Port configuration. Four robotic and two assistant ports. An additional 12 mm suprapubic port is placed to ease restoration of bowel continuity. (B) Identification of the bowel segment. A segment of 45-50 cm of the ileum 15-20 cm proximal to the ileocecal valve is isolated and divided into a right and left limb. (C) Bowel detubularization and construction of the posterior plate. The bowel is detubularized by incising it along its anti-mesenteric border and folded so that the edges of the ascending and descending loop are sutured together. (D) Urethro-ileal anastomosis. Van Velthoven tension-free UIA is performed over a 22 Ch catheter. (E) Closure of the lower half of the anterior wall. Only the lower half of the anterior wall of the neobladder is sutured. (F) Uretero-ileal anastomosis. An end-to-side uretero-ileal anastomosis is made on each chimney after ureteral spatulation. (G) Closure of the anterior wall of the neobladder. The remaining anterior wall of the neobladder is closed in a T-shaped manner.
|
|
|
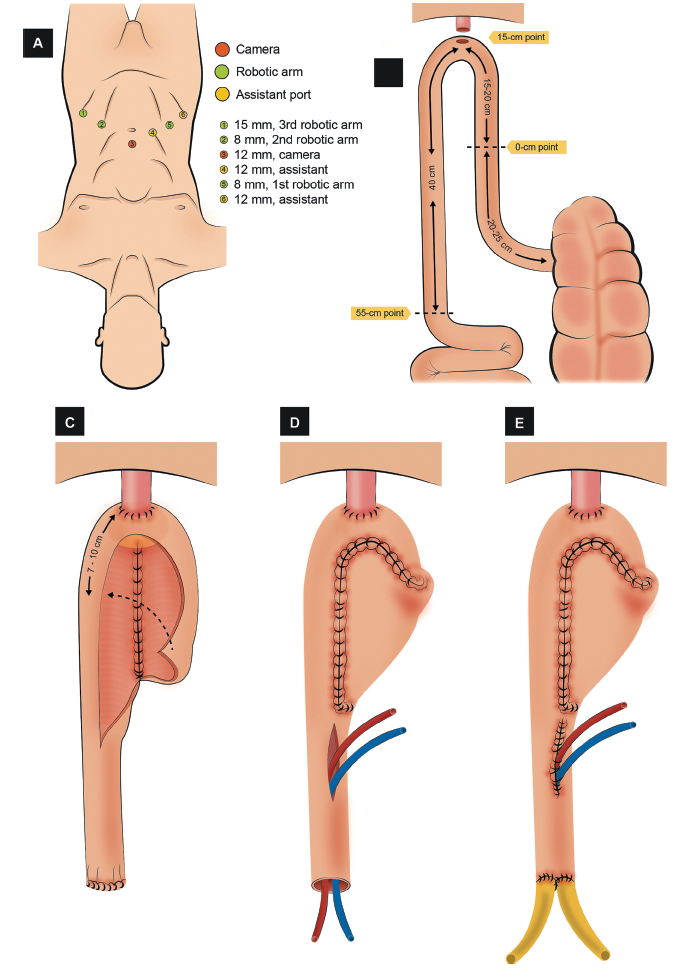
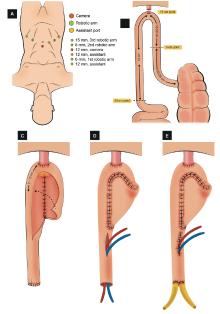
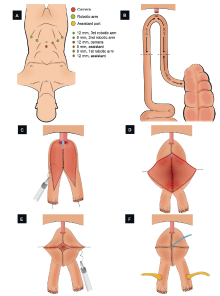
Schematic figure demonstrating the step-by-step creation of the robotic Karolinska-modified Studer “U” ICONB (Adapted from Wiklund and Poulakis [18]). (A) Port configuration. Four robotic and two assistant ports. (B) Identification of the bowel segment. A segment of 55-60 cm of the ileum 20-25 cm proximal to the ileocecal valve is isolated. (C) Construction of the posterior plate and closure of the anterior wall of the neobladder. The intestinal segment is detubularized. The medial edges of the right and left ileal limbs are sutured together to create the posterior plate. The open edge of the right limb is folded anteriorly towards the left limb. The cranial part of the right limb is folded and sutured to the left limb to create the anterior wall. The most proximal part of the anterior wall is kept open to facilitate the passage of ureteral stents. (D) Stent placement. Simple-J ureteric stents introduced through the window in the anterior wall. (E) Uretero-ileal anastomosis and closure of the anterior wall of the neobladder. Wallace anastomosis is made over the ureteric stents, and the window in the anterior wall of the neobladder is closed with a running barbed suture.
|
|
|
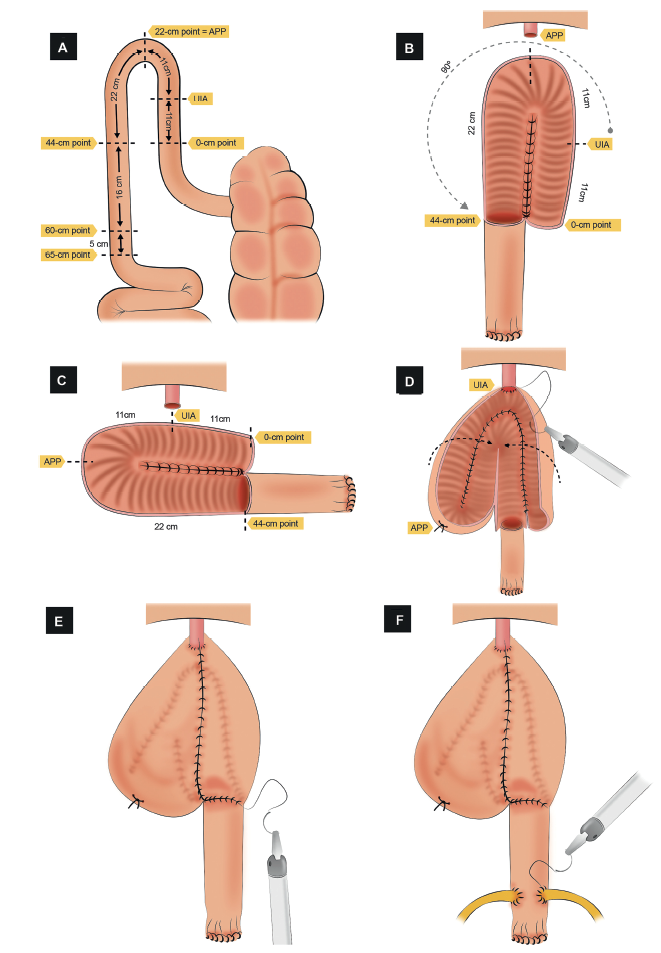
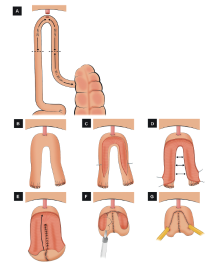
Schematic figure demonstrating the step-by-step creation of the robotic University of Southern California (USC)-modified Studer “U” ICONB (Adapted from Chopra et al. [56]). (A) Identification of the bowel segment. A segment of 65 cm of the ileum is isolated. The most mobile and dependent loop that reaches the urethra is marked as the UIA point. Posteriorly, five separate landmark points are marked. (B) Bowel detubularization, creation of the posterior plate, and rotation. The bowel detubularized (from the 44-cm to 0-cm point) and the medial edges of the matching segments are sutured to create the posterior plate. The posterior plate is rotated 90° counterclockwise. (C) Bowel segment layout after rotation. (D) Urethro-ileal anastomosis and cross folding of the pouch. An urethro-ileal anastomosis is made on the 11-cm point, and the pouch is cross folded to approximate the intestinal edges that will create the anterior wall. (E) Closure of the anterior wall. The cross folded intestinal edges are sutured together to create the anterior wall. (F) Uretero-ileal anastomosis. An end-to-side uretero-ileal anastomosis is performed. APP, apex of the posterior plate; UIA, urethro-ileal anastomosis.
|
|
|
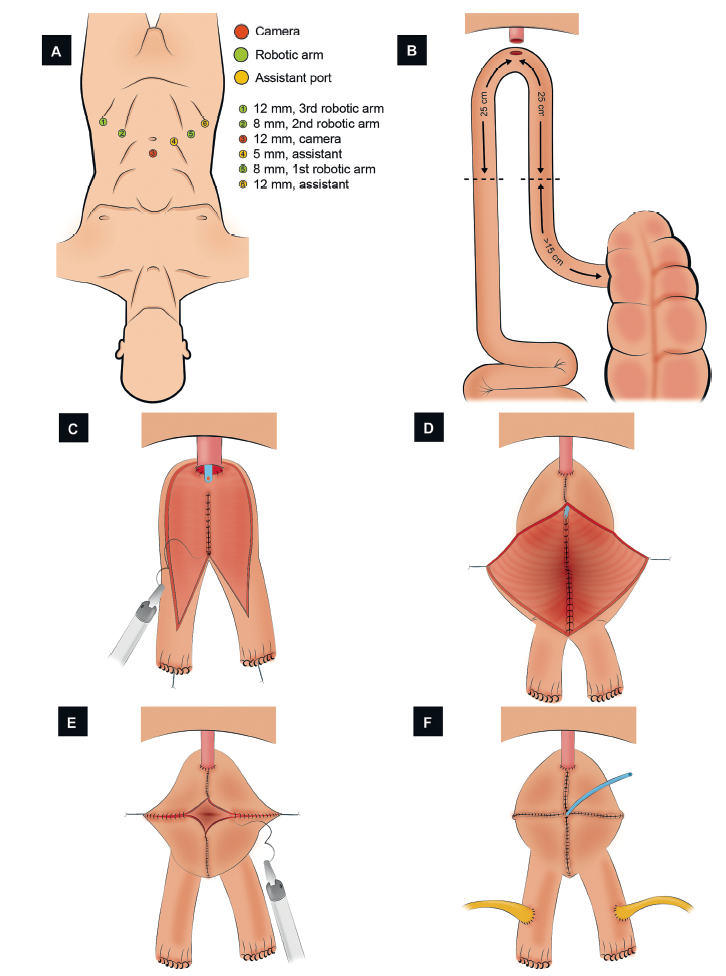
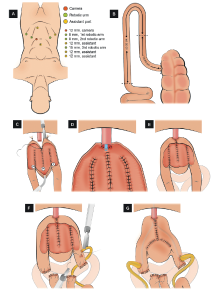
Schematic figure demonstrating the step-by-step creation of the robotic pyramid pouch ICONB (Adapted from Tan et al. [51]). (A) Port configuration. Four robotic and two assistant ports. (B) Identification of the bowel segment. A segment of 50 cm of the ileum >15 cm proximal to the ileocecal valve is isolated. (C) Urethral-ileal anastomosis, bowel detubularization, and formation of the posterior plate. After performing the urethral-ileal anastomosis, the bowel is detubularized (except for the 2 cm uppermost portion of both limbs), and the medial edges of both segments are sutured together. (D) Closure of the distal part of the anterior wall. The first 10 cm of the anterior plate is sutured, from distal to proximal. Two lateral stays are placed in the midway of the remaining bowel segment. (E) Neobladder construction. The closure of the folded bowel was made from lateral to medial in the coronal plane. (F) Uretero-ileal anastomosis. An end-to-side uretero-ileal anastomosis is performed over the proximal end of both ileal limbs.
|
|
|
Schematic figure demonstrating the step-by-step creation of the robotic Y-shaped ICONB (Adapted from Asimakopoulos et al. [47]). (A) Identification of the bowel segment. A segment of 40 cm of the ileum 15-20 cm proximal to the ileocecal valve is isolated. (B) Urethro-ileal anastomosis. After performing the urethro-ileal anastomosis, the ileal segment remains as two ileal limbs. (C) Detubularization of the bowel. The two limbs are detubularized in the antimesenteric border. (D) Construction of the posterior plate. The medial edges of the detubularized limbs are sutured together to create the posterior plate. (E) Folding the pouch. The proximal part of the posterior plate is folded anteriorly. (F) Creation of the anterior wall. The anterior wall is closed with running sutures, creating a “heart shape”. (G) Uretero-ileal anastomosis. An end-to-side uretero-ileal anastomosis is performed over the proximal end of both ileal limbs.
|
|
|
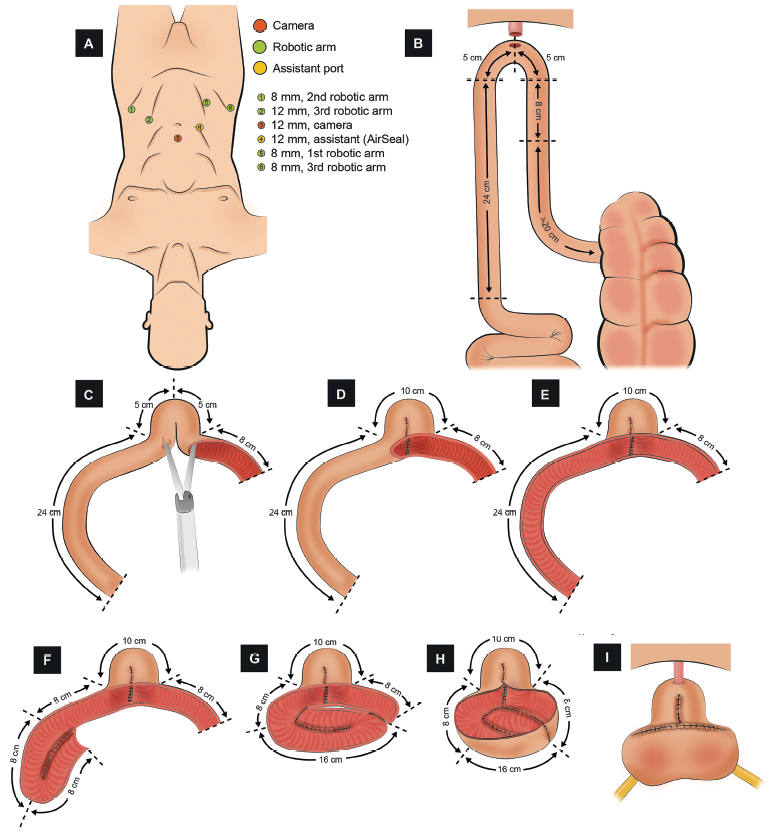
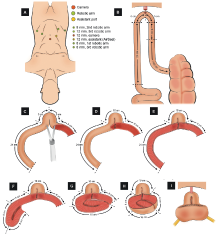
Schematic figure demonstrating the step-by-step creation of the robotic Padua ICONB (Adapted from Simone et al. [48]). (A) Port configuration. Four robotic and two assistant ports. (B) Identification of the bowel segment. A segment of 42 cm of the most dependent portion of the ileum. (C) Detubularization of the distal part of the ileum (8 cm). The most distal part (8 cm) of the small bowel is detubularized (8 cm), and an incision in the left horn is made to insert the stapler. (D) Creation of the neobladder neck. The neobladder neck is created with a stapler. (E) Detubularization of the proximal part of the ileum (24 cm). The remaining ileum (24 cm) is detubularized. (F) First fold. The first 8-cm ileum segment is folded and sutured to the second 8-cm segment. (G) Second fold. The next 8-cm ileum segment is folded over the previous to configure the posterior plate. (H) Completion of the posterior plate of the neobladder. The adjacent edges of the folded ileum are suture together. (I) Urethro-ileal anastomosis, uretero-ileal anastomosis, and completion of the neobladder. A tension-free urethro-ileal anastomosis is performed in the neobladder neck, an end-to-side uretero-ileal anastomosis is performed over the posterior wall, and the neobladder is finally completed with the closure of the anterior wall.
|
| Intestinal segment | Advantages | Disadvantages | | Stomach | ◆ Option for patients with prior pelvic radiotherapy | ◆ Hypokalemic-hypochloremic metabolic alkalosis | | ◆ Beneficial for patients with renal and/or liver dysfunction | ◆ Hematuria-dysuria syndrome | | ◆ Low mucus production | | Jejunum | ◆ Option for patients with prior pelvic radiotherapy | ◆ Hyperkalemic-hypochloremic metabolic acidosis | | ◆ Nausea/vomiting | | Ileum/ileocecum | ◆ More compliant and less contractile than colon and stomach | ◆ Hypokalemic-hyperchloremic metabolic acidosis | | ◆ Fat and bile salt malabsorption | | ◆ Diarrhea | | ◆ Vitamin B12 deficiency | | ◆ Bone demineralization | | Colon | ◆ Option for patients with prior pelvic radiotherapy | ◆ Hypokalemic-hyperchloremic metabolic acidosis, significant mucus production | | ◆ Bone demineralization | | ◆ Pyelonephritis | | ◆ Risk of adenocarcinoma at the anastomosis |
|
|
Comparison of intestinal segments used for the construction of the neobladder (adapted from Tan et al. [60]).
|
| [1] |
Cancer today [Internet]. [accessed Jul 11 2019], http://gco.iarc.fr/today/home.
|
| [2] |
Witjes JA, Bruins M, Cathomas R, Compérat E, Cowan NC, Gakis G, et al. EAU guidelines on muscle-invasive and metastatic bladder cancer. 2019. p. 19-42 [accessed Nov 8 2019], https://uroweb.org/guidelines/.
|
| [3] |
Camey M, Le Duc A. L’enterocystoplastie avec cystoprostatectomie totale pour cancer de la vessie. Ann Urol 1979; 13:114-23.
|
| [4] |
Camey M. Detubularized U-shaped cystoplasty (camey II). Curr Surg Tech Urol 1990; 3:1-7.
|
| [5] |
Hautmann RE, Egghart G, Frohneberg D, Miller K. The ileal neobladder. J Urol 1988; 139:39-42.
|
| [6] |
Studer UE, Ackermann D, Casanova GA, Zingg EJ. Three years’ experience with an ileal low pressure bladder substitute. Br J Urol 1989; 63:43-52.
|
| [7] |
Stein JP, Lieskovsky G, Ginsberg DA, Bochner BH, Skinner DG. The T pouch: an orthotopic ileal neobladder incorporating a serosal lined ileal antireflux technique. J Urol 1998; 159:1836-42.
|
| [8] |
Hauri D. Can gastric pouch as orthotopic bladder replacement be used in adults? J Urol 1996; 156:931-5.
|
| [9] |
Light JK, Engelmann UH. Le bag: total replacement of the bladder using an ileocolonic pouch. J Urol 1986; 136:27-31.
|
| [10] |
M?nsson W, Colleen S. Experience with a detubularized right colonic segment for bladder replacement. Scand J Urol Nephrol 1990; 24:53-6.
|
| [11] |
Reddy PK, Lange PH. Bladder replacement with sigmoid colon after radical cystoprostatectomy. Urology 1987; 29:368-71.
|
| [12] |
Menon M, Hemal AK, Tewari A, Shrivastava A, Shoma AM, El- Tabey NA, et al. Nerve-sparing robot-assisted radical cystoprostatectomy and urinary diversion. BJU Int 2003; 92:232-6.
|
| [13] |
Beecken WD, Wolfram M, Engl T, Bentas W, Probst M, Blaheta R, et al. Robotic-assisted laparoscopic radical cystectomy and intra-abdominal formation of an orthotopic ileal neobladder. Eur Urol 2003; 44:337-9.
|
| [14] |
Pruthi RS, Nix J, McRackan D, Hickerson A, Nielsen ME, Raynor M, et al. Robotic-assisted laparoscopic intracorporeal urinary diversion. Eur Urol 2010; 57:1013-21.
|
| [15] |
Romero-González RJ, López-Verdugo JF, Camacho-Trejo V, Maya-Epelstein A. Robot-assisted laparoscopic radical cystoprostatectomy and construction of totally intraabdominal orthotopic bladder with ileal segment. Initial experience in Mexico. Cir Cir 2011; 79:468-72.
|
| [16] |
Jonsson MN, Adding LC, Hosseini A, Schumacher MC, Volz D, Nilsson A, et al. Robot-assisted radical cystectomy with intracorporeal urinary diversion in patients with transitional cell carcinoma of the bladder. Eur Urol 2011; 60:1066-73.
|
| [17] |
Hosseini A, Adding C, Nilsson A, Jonsson MN, Wiklund NP. Robotic cystectomy: surgical technique. BJU Int 2011; 108:962-8.
|
| [18] |
Wiklund NP, Poulakis V. Robotic neobladder. BJU Int 2011; 107:1514-37.
|
| [19] |
Akbulut Z, Canda AE, Ozcan MF, Atmaca AF, Ozdemir AT, Balbay MD. Robot-assisted laparoscopic nerve-sparing radical cystoprostatectomy with bilateral extended lymph node dissection and intracorporeal studer pouch construction: outcomes of first 12 cases. J Endourol 2011; 25:1469-79.
|
| [20] |
Schumacher MC, Jonsson MN, Hosseini A, Nyberg T, Poulakis V, Pardalidis NP, et al. Surgery-related complications of robotassisted radical cystectomy with intracorporeal urinary diversion. Urology 2011; 77:871-6.
|
| [21] |
Goh AC, Gill IS, Lee DJ, de Castro Abreu AL, Fairey AS, Leslie S, et al. Robotic intracorporeal orthotopic ileal neobladder: replicating open surgical principles. Eur Urol 2012; 62:891-901.
|
| [22] |
Canda AE, Atmaca AF, Altinova S, Akbulut Z, Balbay MD. Robot-assisted nerve-sparing radical cystectomy with bilateral extended pelvic lymph node dissection (PLND) and intracorporeal urinary diversion for bladder cancer: initial experience in 27 cases. BJU Int 2012; 110:434-44.
|
| [23] |
Haddad RL, Richard P, Bladou F. Canada's first robotic-assisted totally intracorporeal orthotopic ileal neobladder. Can Urol Assoc J 2013; 7:E537-42.
|
| [24] |
Collins JW, Tyritzis S, Nyberg T, Schumacher M, Laurin O, Khazaeli D, et al. Robot-assisted radical cystectomy: description of an evolved approach to radical cystectomy. Eur Urol 2013; 64:654-63.
|
| [25] |
Tyritzis SI, Hosseini A, Collins J, Nyberg T, Jonsson MN, Laurin O, et al. Oncologic, functional, and complications outcomes of robot-assisted radical cystectomy with totally intracorporeal neobladder diversion. Eur Urol 2013; 64:734-41.
|
| [26] |
Desai MM, de Abreu ALC, Goh AC, Fairey A, Berger A, Leslie S, et al. Robotic intracorporeal urinary diversion: technical details to improve time efficiency. J Endourol 2014; 28:1320-7.
|
| [27] |
Collins JW, Sooriakumaran P, Sanchez-Salas R, Ahonen R, Nyberg T, Wiklund NP, et al. Robot-assisted radical cystectomy with intracorporeal neobladder diversion: the Karolinska experience. Indian J Urol 2014; 30:307-13.
|
| [28] |
Abreu AL de C, Chopra S, Azhar RA, Berger AK, Miranda G, Cai J, et al. Robotic radical cystectomy and intracorporeal urinary diversion: the USC technique. Indian J Urol 2014; 30:300-6.
|
| [29] |
Butt ZA, Forbes E, Zorn J, Martin BS. Robotic radical cystectomy with intracorporeal neobladder: initial experience and outcomes. Can Urol Assoc J 2015; 9:E156-9. https://doi.org/10.5489/cuaj.2193.
|
| [30] |
Atmaca AF, Canda AE, Gok B, Akbulut Z, Altinova S, Balbay MD. Open versus robotic radical cystectomy with intracorporeal Studer diversion. J Soc Laparoendosc Surg 2015; 19:e2014.00193. https://doi.org/10.4293/JSLS.2014.00193.
|
| [31] |
Schwentner C, Sim A, Balbay MD, Todenh?fer T, Aufderklamm S, Halalsheh O, et al. Robot-assisted radical cystectomy and intracorporeal neobladder formation: on the way to a standardized procedure. World J Surg Oncol 2015; 13:3. https://doi.org/10.1186/1477-7819-13-3.
pmid: 26596801
|
| [32] |
Desai MM, Gill IS, de Castro Abreu AL, Hosseini A, Nyberg T, Adding C, et al. Robotic intracorporeal orthotopic neobladder during radical cystectomy in 132 patients. J Urol 2014; 192:1734-40.
|
| [33] |
Koupparis A, Villeda-Sandoval C, Weale N, El-Mahdy M, Gillatt D, Rowe E. Robot-assisted radical cystectomy with intracorporeal urinary diversion: impact on an established enhanced recovery protocol. BJU Int 2015; 116:924-31.
|
| [34] |
Nyame YA, Zargar H, Ramirez D, Ganesan V, Babbar P, Villers A, et al. Robotic-assisted laparoscopic bilateral nervesparing and apex preserving cystoprostatectomy in young men with bladder cancer. Urology 2016; 94:259-64.
|
| [35] |
Almassi N, Zargar H, Ganesan V, Fergany A, Haber GP. Management of challenging urethro-ileal anastomosis during robotic assisted radical cystectomy with intracorporeal neobladder formation. Eur Urol 2016; 69:704-9.
|
| [36] |
Satkunasivam R, Santomauro M, Chopra S, Plotner E, Cai J, Miranda G, et al. Robotic intracorporeal orthotopic neobladder: urodynamic outcomes, urinary function, and health-related quality of life. Eur Urol 2016; 69:247-53.
|
| [37] |
Koie T, Ohyama C, Yoneyama T, Nagasaka H, Yamamoto H, Imai A, et al. Robotic cross-folded U-configuration intracorporeal ileal neobladder for muscle-invasive bladder cancer: initial experience and functional outcomes. Int JMed Robot 2018; 14:e1955. https://doi.org/10.1002/rcs.1955.
|
| [38] |
Sim A, Balbay MD, Todenh?fer T, Aufderklamm S, Halalsheh O, Mischinger J, et al. Robot-assisted radical cystectomy and intracorporeal urinary diversiondsafe and reproducible? Cent Eur J Urol 2015; 68:18-23.
|
| [39] |
Porreca A, Chessa F, Romagnoli D, Salvaggio A, Cafarelli A, Borghesi M, et al. Robot assisted radical cystectomy with totally intracorporeal urinary diversion: initial, single-surgeon’s experience after a modified modular training. Minerva Urol Nefrol 2018; 70:193-201.
|
| [40] |
Chow K, Zargar H, Corcoran NM, Costello AJ, Peters JS, Dundee P. Robotic-assisted radical cystectomy with intracorporeal urinary diversion versus open: early Australian experience. ANZ J Surg 2018; 88:1028-32.
|
| [41] |
Lenfant L, Verhoest G, Campi R, Parra J, Graffeille V, Masson- Lecomte A, et al. Perioperative outcomes and complications of intracorporeal vs. extracorporeal urinary diversion after robot-assisted radical cystectomy for bladder cancer: a reallife, multi-institutional French study. World J Urol 2018; 36:1711-8.
|
| [42] |
Porreca A, Mineo Bianchi F, Romagnoli D, D’Agostino D, Corsi P, Giampaoli M, et al. Robot-assisted radical cystectomy with totally intracorporeal urinary diversion: surgical and early functional outcomes through the learning curve in a single high-volume center. J Robot Surg 2020; 14:261-9.
|
| [43] |
Brassetti A, Cacciamani G, Anceschi U, Ferriero M, Tuderti G, Miranda G, et al. Long-term oncologic outcomes of robotassisted radical cystectomy (RARC) with totally intracorporeal urinary diversion (ICUD): a multi-center study. World J Urol 2020; 38:837-43.
|
| [44] |
Sala LG, Matsunaga GS, Corica FA, Ornstein DK. Robot-assisted laparoscopic radical cystoprostatectomy and totally intracorporeal ileal neobladder. J Endourol 2006; 20:233-6.
|
| [45] |
Hussein AA, Ahmed YE, Kozlowski JD, May PR, Nyquist J, Sexton S, et al. Robot-assisted approach to ‘W’-configuration urinary diversion: a step-by-step technique. BJU Int 2017; 120:152-7.
|
| [46] |
Sim A, Todenh?fer T, Mischinger J, Halalsheh O, Fahmy O, Boettge J, et al. Y pouch neobladderda simplified method of intracorporeal neobladder after robotic cystectomy. J Endourol 2015; 29:387-9.
|
| [47] |
Asimakopoulos AD, Campagna A, Gakis G, Corona Montes VE, Piechaud T, Hoepffner JL, et al. Nerve-sparing, robot-assisted radical cystectomy with intracorporeal bladder substitution in the male. J Urol 2016; 196:1549-57.
|
| [48] |
Simone G, Papalia R, Misuraca L, Tuderti G, Minisola F, Ferriero M, et al. Robotic intracorporeal padua Ileal bladder: surgical technique, perioperative, oncologic and functional outcomes. Eur Urol 2018; 73:934-40.
|
| [49] |
Simone G, Tuderti G, Misuraca L, Anceschi U, Ferriero M, Minisola F, et al. Perioperative and mid-term oncologic outcomes of robotic assisted radical cystectomy with totally intracorporeal neobladder: results of a propensity score matched comparison with open cohort from a single-centre series. Eur J Surg Oncol 2018; 44:1432-8.
|
| [50] |
Kang SG, Ko YH, Jang HA, Kim J, Kim SH, Cheon J, et al. Initial experience of robot-assisted radical cystectomy with total intracorporeal urinary diversion: comparison with extracorporeal method. J Laparoendosc Adv Surg Tech 2012; 22:456-62.
|
| [51] |
Tan WS, Sridhar A, Goldstraw M, Zacharakis E, Nathan S, Hines J, et al. Robot-assisted intracorporeal pyramid neobladder. BJU Int 2015; 116:771-9.
|
| [52] |
Cacciamani GE, de Marco V, Sebben M, Rizzetto R, Cerruto MA, Porcaro AB, et al. Robot-assisted Vescica Ileale Padovana: a new technique for intracorporeal bladder replacement reproducing open surgical principles. Eur Urol 2019; 76:381-90.
|
| [53] |
Minervini A, Vanacore D, Vittori G, Milanesi M, Tuccio A, Siena G, et al. Florence robotic intracorporeal neobladder (FloRIN): a new reconfiguration strategy developed following the IDEAL guidelines. BJU Int 2018; 121:313-7.
|
| [54] |
Hussein AA, May PR, Jing Z, Ahmed YE, Wijburg CJ, Canda AE, et al. Outcomes of intracorporeal urinary diversion after robot-assisted radical cystectomy: results from the international robotic cystectomy consortium. J Urol 2018; 199:1302-11.
|
| [55] |
Studer UE, Turner WH. The ileal orthotopic bladder. Urology 1995; 45:185-9.
|
| [56] |
Chopra S, de Castro Abreu AL, Berger AK, Sehgal S, Gill I, Aron M, et al. Evolution of robot-assisted orthotopic ileal neobladder formation: a step-by-step update to the University of Southern California (USC) technique. BJU Int 2017; 119:185-91.
|
| [57] |
Borirakchanyavat S, Aboseif SR, Carroll PR, Tanagho EA, Lue TF. Continence mechanism of the isolated female urethra: an anatomical study of the intrapelvic somatic nerves. J Urol 1997; 158:822-6.
|
| [58] |
Colleselli K, Stenzl A, Eder R, Strasser H, Poisel S, Bartsch G. The female urethral sphincter: a morphological and topographical study. J Urol 1998; 160:49-54.
|
| [59] |
Hinman F. Selection of intestinal segments for bladder substitution: physical and physiological characteristics. J Urol 1988; 139:519-23.
|
| [60] |
Tan WS, Lamb BW, Kelly JD. Evolution of the neobladder: a critical review of open and intracorporeal neobladder reconstruction techniques. Scand J Urol 2016; 50:95-103.
|
| [1] |
Hugo Otaola-Arca,Rafael Coelho,Vipul R. Patel,Marcelo Orvieto. Totally intracorporeal robot-assisted urinary diversion for bladder cancer (Part 1). Review and detailed characterization of ileal conduit and modified Indiana pouch[J]. Asian Journal of Urology, 2021, 8(1): 50-62. |
| [2] |
Marcio Covas Moschovas,Kulthe Ramesh Seetharam Bhat,Cathy Jenson,Vipul R. Patel,Gabriel Ogaya-Pinies. Robtic-assisted radical cystectomy: Literature review[J]. Asian Journal of Urology, 2021, 8(1): 14-19. |
| [3] |
Kulthe Ramesh Seetharam Bhat,Marcio Covas Moschovas,Vipul R. Patel,Young Hwii Ko. The robot-assisted ureteral reconstruction in adult: A narrative review on the surgical techniques and contemporary outcomes[J]. Asian Journal of Urology, 2021, 8(1): 38-49. |
| [4] |
Tripathi Abhishek,Gupta Shilpa. Androgen receptor in bladder cancer: A promising therapeutic target[J]. Asian Journal of Urology, 2020, 7(3): 284-290. |
| [5] |
Xie Weibin,Bi Junming,Wei Qiang,Han Ping,Song Dongkui,Shi Lei,Ye Dingwei,Shen Yijun,Gou Xin,He Weiyang,Wang Shaogang,Liu Zheng,Fan Jinhai,Wu Kaijie,Chen Zhiwen,Zhou Xiaozhou,Kong Chuize,Liu Yang,Liu Chunxiao,Xu Abai,Jin Baiye,Fu Guanghou,Xue Wei,Chen Haige,Pan Tiejun,Tu Zhong,Lin Tianxin,Huang Jian. Survival after radical cystectomy for bladder cancer: Multicenter comparison between minimally invasive and open approaches[J]. Asian Journal of Urology, 2020, 7(3): 291-300. |
| [6] |
Guido Barbagli,Axel Heidenreich,Vahudin Zugor,Leonidas Karapanos,Massimo Lazzeri. Urothelial or oral mucosa cells for tissue-engineered urethroplasty: A critical revision of the clinical outcome[J]. Asian Journal of Urology, 2020, 7(1): 18-23. |
| [7] |
Sunny Goel,Rahul J. Sinha,Ved Bhaskar,Ruchir Aeron,Ashish Sharma,Vishwajeet Singh. Role of gemcitabine and cisplatin as neoadjuvant chemotherapy in muscle invasive bladder cancer: Experience over the last decade[J]. Asian Journal of Urology, 2019, 6(3): 222-229. |
| [8] |
Yifan Chang,Xiaojun Lu,Qingliang Zhu,Chuanliang Xu,Yinghao Sun,Shancheng Ren. Single-port transperitoneal robotic-assisted laparoscopic radical prostatectomy (spRALP): Initial experience[J]. Asian Journal of Urology, 2019, 6(3): 294-297. |
| [9] |
Gild Philipp,A. Kluth Luis,W. Vetterlein Malte,Engel Oliver,K.H. Chun Felix,Fisch Margit. Adult iatrogenic ureteral injury and stricture-incidence and treatment strategies[J]. Asian Journal of Urology, 2018, 5(2): 101-106. |
| [10] |
Ka Wing Wong, Terence Chun-ting Lai, Ada Tsui-lin Ng, Brian Sze-ho Ho, James Hok-leung Tsu, Chiu Fung Tsang, W. K. Ma, Ming Kwong Yiu. Anterior perineal hernia after anterior exenteration[J]. Asian Journal of Urology, 2017, 4(4): 253-255. |
| [11] |
Yu Guang Tan, Ernest Eu, Weber Lau Kam On, Hong Hong Huang. Pretreatment neutrophil-to-lymphocyte ratio predicts worse survival outcomes and advanced tumor staging in patients undergoing radical cystectomy for bladder cancer[J]. Asian Journal of Urology, 2017, 4(4): 239-246. |
| [12] |
David J. McConkey, Woonyoung Choi, Andrea Ochoa, Colin P. N. Dinney. Intrinsic subtypes and bladder cancer metastasis[J]. Asian Journal of Urology, 2016, 3(4): 260-267. |
| [13] |
Wei Wang, Haitao Liu, Shujie Xia. Thulium laser treatment for bladder cancer[J]. Asian Journal of Urology, 2016, 3(3): 130-133. |
| [14] |
Thomas Y. Hsueh, Allen W. Chiu. Narrow band imaging for bladder cancer[J]. Asian Journal of Urology, 2016, 3(3): 126-129. |
| [15] |
Kaiwen Li, Tianxin Lin, Chinese Bladder Cancer Consortium, Wei Xue, Xin Mu, Enci Xu, Xu Yang, Fubao Chen, Guangyong Li, Lulin Ma, Guoliang Wang, Chaozhao Liang, Haoqiang Shi, Ming Li, Mao Tang, Xueyi Xue, Yisong Lv, Yaoliang Deng, Chengyang Li, Zhiwen Chen, Xiaozhou Zhou, Fengshuo Jin, Xudong Liu, Jinxin Wei, Lei Shi, Xin Gou, Weiyang He, Liqun Zhou, Lin Cai, Liping Xie, Guanghou Fu, Xiangbo Kong, Hongyan Sun, Ye Tian, Lang Feng, Tiejun Pan, Yiyi Wu, Dongwen Wang, Hailong Hao, Benkang Shi, Yaofeng Zhu, Qiang Wei, Ping Han, Changli Wu, Dawei Tian, Zhangqun Ye, Zheng Liu, Zhiping Wang, Junqiang Tian, Lin Qi, Minfeng Chen, Wei Li, Jinchun Qi, Gongxian Wang, Longlong Fu, Zhaolin Sun, Guangheng Luo, Zhoujun Shen, Zhaowei Zhu, Jinchun Xing, Zhun Wu, Dong Wei, Xin Chen, Yanqun Na, Hongfeng Guo, Chunxi Wang, Zhihua Lu, Chuize Kong, Yang Liu, Jin Yang, Jianyun Hu, Xin Gao, Jielin Li, Changjun Yin, Pu Li, Shan Chen, Zhen Du, Jiongming Li, Yongji Yan, Xu Zhang, Shuang Huang, Fangjian Zhou, Zhiling Zhang, Yinghao Sun, Shuxiong Zeng, Song Cen, Jiaquan Zhou, Hanzhong Li, Jin Wen, Jian Huang. Current status of diagnosis and treatment of bladder cancer in China-Analyses of Chinese Bladder Cancer Consortium Database[J]. Asian Journal of Urology, 2015, 2(2): 63-69. |
|
|
|
|