|
|
|
| Robot-assisted retroperitoneal lymphadenectomy: The state of art |
Gilberto J. Rodriguesa,Giuliano B. Guglielmettia,Marcelo Orvietob,Kulthe Ramesh Seetharam Bhatc,Vipul R. Patelc,Rafael F. Coelhoa,*( ) )
|
a Sao Paulo State Cancer Institute, University of Sao Paulo School of Medicine, Sao Paulo, Brazil
b Clínica Alemana, Santiago, Chile
c Department of Urology, AdventHealth Global Robotics Institute, Celebration, FL, United States |
|
|
|
|
Abstract Objective: To perform a narrative review about the role of robot-assisted retroperitoneal lymphadenectomy (R-RPLND) in the management of testicular cancer. Methods: A PubMed search for all relevant publications regarding the R-RPLND series up until August 2019 was performed. The largest series were identified, and weighted means calculated for outcomes using the number of patients included in each study as the weighting factor. Results: Fifty-six articles of R-RPLND were identified and eight series with more than 10 patients in each were included. The weighted mean age was 31.12 years; primary and post chemotherapy R-RPLND were performed in 50.59% and 49.41% of patients. The clinical stage was I, II and III in 47.20%, 39.57% and 13.23% of patients. A modified R-RPLND template was used in 78.02% of patients, while 21.98% underwent bilateral full template. The weighted mean node yield, operative time and estimated blood loss were, respectively, 22.15 nodes, 277.35 min and 131.94 mL. The weighted mean length of hospital stay was 2 days and antegrade ejaculation was preserved in 92.12% of patients. Major post-operative complications (Clavien III or IV) occurred in 5.34%. Positive pathological nodes were detected in 24.54%, while the recurrence free survival was 95.77% with a follow-up of 21.81 months. Conclusion: R-RPLND has proven to be a reproducible and safe approach in experienced centers; short-term oncologic outcomes are similar to the open approach with less morbidity and shorter convalescence related to its minimal invasiveness. However, longer follow-up and new trials comparing head-to-head both techniques are expected.
|
|
Received: 17 February 2020
Available online: 20 January 2021
|
|
Corresponding Authors:
Rafael F. Coelho
E-mail: coelhouro@yahoo.com.br
|
|
|
|
|
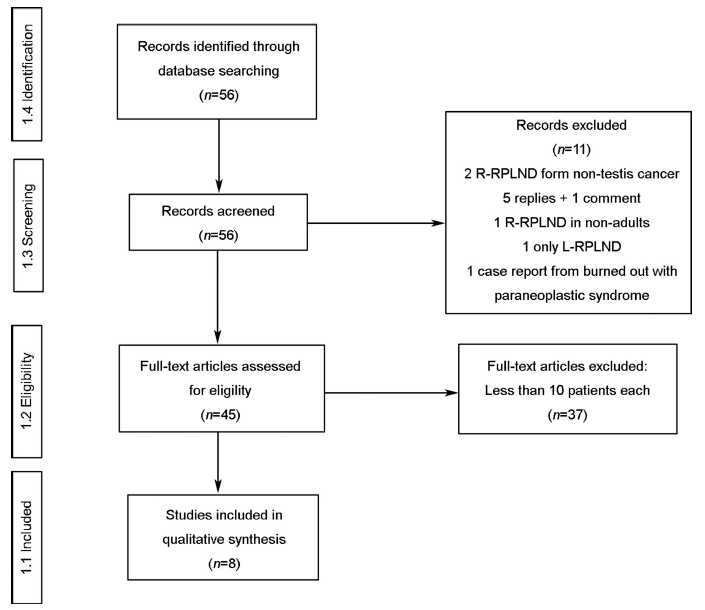
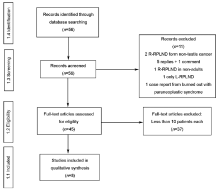
PRISMA 2009 Flow Diagram. R-RPLND, robot-assisted retroperitoneal lymphadenectomy; L-RPLND, laparoscopic retroperitoneal lymph node dissection; PRISMA, the Preferred Reporting Items for Systematic Reviews and Meta-Analyses. From: Moher D, Liberati A, Tetzlaff J, Altman DG, the PRISMA Group (2009). Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med 6 (7): e1000097. https://doi.org/10.1371/journal.pmed1000097. For more information, visit http://www.prisma-statement.org/.
|

| Scenario | Pearce et al., 2017 [13] | Harris et al., 2015 [14] | Stepanian et al., 2016 [10] | Cheney et al., 2015 [15] | Li et al., 2019 [18] | Singh et al., 2017 [11] | Kamel et al., 2016 [17] | Overs et al., 2018 [16] | Weighted means | | pR-RPLND | pR-RPLND and PC-R-RPLND | PC-R-RPLND | | Median age, years (IQR) | 30 (26-38) | 30 (25-38) | 31 | 35 (23-39) | 30 (26-36) | 26 (21-37) | 38 (20-55) | 33 (22-49) | 31.12 | | Number of patients | 47 | 16 | 20 | 18 | 30 | 13 | 12 | 11 | 27.08 | | pR-RPLND n (%) | 47 (100) | 16 (100) | 16 (75) | 11 (36) | 0 | 0 | 0 | 0 | 50.59% | | PC-R-RPLND, n (%) | 0 | 0 | 4 (25) | 7 (64) | 30 (100) | 13 (100) | 12 (100) | 11 (100) | 49.41% | | cTNM Stage n (%) | | I | 42 (89) | 16 (100) | 11 (55) | 10 (56) | 0 | 0 | 0 | 0 | 47.20% | | II | 5 (11) | 0 | 6 (30) | 7 (39) | 19 (63) | 13 (100) | 6 (50) | 10 (91) | 39.57% | | III | 0 | 0 | 3 (15) | 1 (6) | 11 (37) | 0 | 6 (50) | 1 (9) | 13.23% |
|
|
Characteristics of patients and scenario from the largest series of R-RPLND with the weighted means calculated.
|
| Scenario | Pearce et al., 2017 [13] | Harris et al., 2015 [14] | Stepanian et al., 2016 [10] | Cheney et al., 2015 [15] | Li et al., 2019 [18] | Singh et al., 2017 [11] | Kamel et al., 2016 [17] | Overs et al., 2018 [16] | Weighted means | | pR-RPLND | pR-RPLND and PC-R-RPLND | PC-R-RPLND | | Patient positioning-robot docking, n (%) | | Flank-lateral | 42 (89) | 16 (100) | 11 (55) | 0 | 30 (100) | 12 (92) | 6 (50) | 11 (100) | 76.52% | | Supine-cranial | 5 (11)a | 0 | 9 (45) | 18 (100) | 0 | 1 (8) | 6 (50) | 0 | 23.48% | | RPLND template, n (%) | | Modified | 45 (96) | 16 (100) | 14 (70) | 7 (39) | 17 (57) | 11 (85) | 9 (75) | 11 (100) | 78.02% | | Bilateral | 2 (4) | 0 | 6 (30) | 11 (61) | 13 (43) | 2 (15) | 3 (25) | 0 | 21.98% | | Node yield | 26 (18-32)b | 30 (23-36)b | 20 (14-27)b | 22 (10)c | 24 (17-30)b | 20d | 12 (5-21)e | 7 (1; 24)f | 22.15 | | Operative time, min | 235 (214-258)b | 271 (236-299)b | 293 (258-317)b | 329 (40)c | 372 (329-437)b | 200d | 312 (205-408)e | 150 (45-300)e | 277.35 | | Estimated blood loss, mL, | 50 (50-100)b | 75 (50-100)b | 50 (50-100)b | 103 (78)c | 235 (160-300)b | 120d | 475 (50-1800)e | 120 (5-300)f | 131.94 | | Length of stay, day | 1 (1-1)b | NR | 1 (1-2)b | 3 (2.3)c | 2d | 4 (3-5)b | 3 (2-5)e | 3 (2-4)f | 2.00 |
|
|
Operative outcomes from the eight largest series of R-RPLND with the weighted means calculated.
|
| Scenario | Pearce et al., 2017 [13] | Harris et al., 2015 [14] | Stepanian et al., 2016 [10] | Cheney et al., 2015 [15] | Li et al., 2019 [18] | Singh et al., 2017 [11] | Kamel et al., 2016 [17] | Overs et al., 2018 [16] | Weighted means | | pR-RPLND | pR-RPLND and PC-R-RPLND | PC-R-RPLND | | Complications | | Overall, n (%) | 6 (13) | 1 (6) | 1 (5) | 6 (33) | 10 (33) | 10 (77) | 5 (42) | 1 (9) | 23.92% | | Trans-operative, n (%) | 2 (4) | 1 (6) | 1 (5) | 3 (17) | 4 (13) | 1 (8) | 2 (17) | 0 | 8.31% | | Injury, no conversion | 1 pancreatic | 0 | 1 ureter | 0 | 1 diaphragmatic | 1 aortic | 1 aortic | 0 | NA | | Conversion, n (%) | 1 (2) | 1 (6) | 0 | 3 (17) | 3 (10) | 0 | 1 (8) | 0 | 5.34% | | Reason | 1 aortic injury | 1 aortic injury | 0 | 1 robotic malfunction
1 poor exposure
1 risk of bleeding | 2 poor visualization
1 vascular injury | 0 | 1 inferior mesenteric artery injury | 0 | NA | | Post-operative, ≤90 day, n (%) | 4 (9) | 0 | 0 | 3 (17) | 6 (20) | 9 (69) | 3 (25) | 1 (9) | 15.19% | | Clavien-Dindo I-II | 1 chylous ascites
1 ileus | 0 | 0 | 1 ileus
1 transfusion
1 hyperkalemia | 2 wound infection
1 delirium tremens | 5 ileus
1 chylous ascites | 1 ileus
1 neuropathy in the upper limb | 1 chylous ascites | 9.80% | | Clavien-Dindo III-IV | 1 chylous ascites
1 body wall hematoma | 0 | 0 | 0 | 1 chylous ascites
1 colon perforation leading to multiple organ failure
1 pneumothorax | 3 chylous ascites | 1 aortic pseudoaneurysm repaired by endovascular technique | 0 | 5.39% |
|
|
Complications from the largest series of R-RPLND with the weighted means calculated.
|
| Scenario | Pearce et al., 2017 [13] | Harris et al., 2015 [14] | Stepanian et al., 2016 [10] | Cheney et al., 2015 [15] | Li et al., 2019 [18] | Singh et al.,
2017 [11] | Kamel et al., 2016 [17] | Overs et al., 2018 [16] | Weighted means | | pR-RPLND | pR-RPLND and PC-R-RPLND | PC-R-RPLND | | Antegrade ejaculation, n (%) | | No | 0 | 0 | 2 (10) | 1 (9)d | 0 | 2 (15) | 1 (10)f | 1 (11)f | NA | | Yes | 44 (94) | 16 (100) | 18 (90) | 10 (91)d | 0 | 11 (85) | 9 (90)f | 8 (89)f | 92.12% | | Unknown | 3 (6) | 0 | 0 | 0 | 30 (100) | 0 | 2 (17) | 2 (18) | NA | | Patients pN+a, n (%) | 8 (17) | 2 (13) | 8 (42) | 8 (44) | 5 (17) | 3 (23) | 5 (46) | 1 (9)g | 24.54% | | Adjuvant chemotherapy (if pN+), n (%) | | No | 3 (38) | NR | 18 (90) | 16 (89) | 3 (17) | 13 (100) | 0 | 11 (100) | NA | | Yes | 5 (62) | NR | 2 (10) | 2 (11) | 2 (7) | 0 | 1 (8) | 0 | 23.96% | | Recurrence | | In-field recurrence, n | 0 | NR | 0 | 0 | 0 | 0 | 0 | 0 | NA | | RFSb, % | 97 | NR | 100 | 89 | 90 | 100 | 100 | 100 | 95.77 | | Follow-up, month | 16 (9-23)c | NR | 49 (37-71)c | 22 (1-58)c | 15 (1-51)e | 23 (3-58)e | 31 (5-39)e | 4 (1-48)e | 21.81 |
|
|
Functional and oncological outcomes from the largest series of R-RPLND with the weighted means calculated.
|
|
|
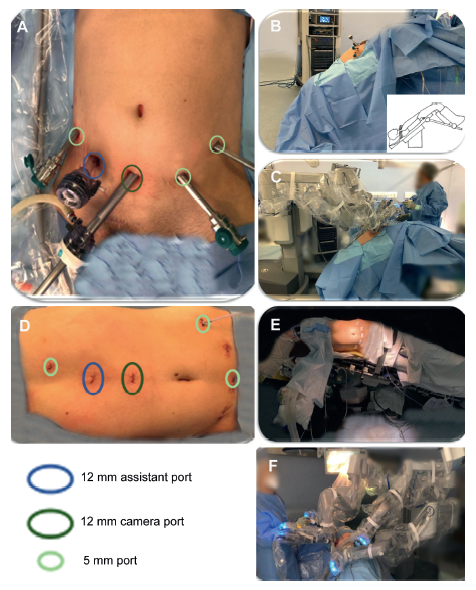
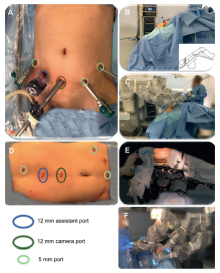
Supine position and docking and flank position and docking. (A) Trocar placement; (B) Patient positioning; (C) Robot docking; (D) Supine; (E) Flank decubitus; (F) The doctors were performing R-RPLND. R-RPLND, robot-assisted retroperitoneal lymphadenectomy.
|
|
|
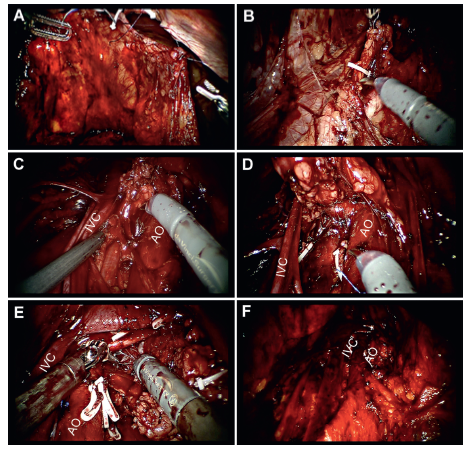
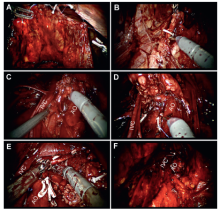
Trans-operative relevant moments of RPLND in supine position. (A) Peritoneum suspension in abdominal wall to begin dissection and access the retroperitoneum; (B) Beginning of paracaval template, above the ureter cross the right iliac artery; (C) Precaval, preaortic, interaortocaval and retrocaval template with identification and sparing of postganglionic sympathetic nerve fibers (crossing between the IVC and AO); (D) Interaortocaval and retrocaval dissection reaching the right superior boundaries of the template (right renal hilum); (E) Preaortic and paraortic superior boundaries reaching the left renal hilum; (F) Final template showing the retroperitoneum vessels. AO, aorta; IVC, inferior vena cava; RPLND, retroperitoneal lymph node dissection.
|
|
|
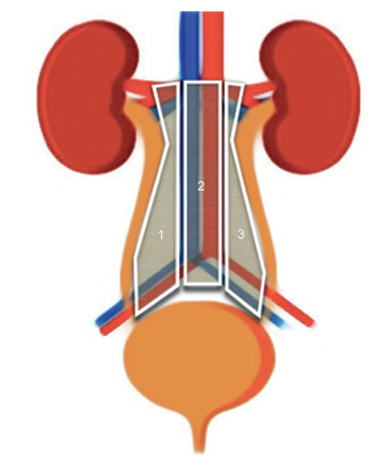
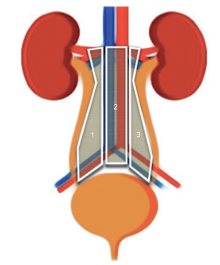
Schematic templates and boundaries for retroperitoneal lymphadenectomy. 1. Boundaries of paracaval template (superior: Right renal hilum including dissection of renal arteries; lateral: Right ureter; medial: Interaortocaval template; inferior: Right ureter crossing the right iliac vessels. 2. Boundaries of interaortocaval, precaval, retrocaval, preaortic and retroaortic templates (superior: Renal vessels; lateral: Paracaval and paraortic templates; inferior: Aorta bifurcation. 3. Boundaries of paraaortic template (superior: Left renal hilum including dissection of renal arteries; lateral: Left ureter; inferior: Left ureter crossing the left iliac vessels [laterally]).
|
| [1] |
Schwen ZR, Gupta M, Pierorazio PM. A review of outcomes and technique for the robotic-assisted laparoscopic retroperitoneal lymph node dissection for testicular cancer. Adv Urol 2018; 2018:2146080. https://doi.org/10.1155/2018/2146080.
pmid: 29853869
|
| [2] |
Laguna MP, Albers P, Algaba F, Bokemeyer C, Boormans JL, Fischer S, et al. EAU guidelines: testicular cancer. [Accessed 2 September 2019]. https://uroweb.org/guideline/testicularcancer/.
|
| [3] |
Ahluwalia P, Gautam G. Current concepts in management of stage I NSGCT. Indian J Surg Oncol 2017; 8:51-8.
|
| [4] |
Williams SB, Lau CS, Josephson DY. Initial series of robotassisted laparoscopic retroperitoneal lymph node dissection for clinical stage I nonseminomatous germ cell testicular cancer. Eur Urol 2011; 60:1299-302.
|
| [5] |
Rassweiler JJ, Teber D. Advances in laparoscopic surgery in urology. Nat Rev Urol 2016; 13:387-99.
|
| [6] |
Rukstalis DB, Chodak GW. Laparoscopic retroperitoneal lymph node dissection in a patient with stage 1 testicular carcinoma. J Urol 1992; 148:1907-10.
|
| [7] |
?slamo?lu E, ?zsoy ?, An?l H, Akta? Y, Ate? M, Sava? M. Postchemotherapy robot-assisted retroperitoneal lymph node dissection in non-seminomatous germ cell tumor of testis: feasibility and outcomes of initial cases. Turk J Urol 2018; 45:113-7.
|
| [8] |
Davol P, Sumfest J, Rukstalis D. Robotic-assisted laparoscopic retroperitoneal lymph node dissection. Urology 2006; 67:199. https://doi.org/10.1016/j.urology.2005.07.022.
pmid: 16413365
|
| [9] |
Pugin F, Bucher P, Morel P. History of robotic surgery: from AESOP? and ZEUS? to da Vinci?. J Visc Surg 2011;148(5 Suppl): e3-8. https://doi.org/10.1016/j.jviscsurg.2011.04.007.
|
| [10] |
Stepanian S, Patel M, Porter J. Robot-assisted laparoscopic retroperitoneal lymph node dissection for testicular cancer: evolution of the technique. Eur Urol 2016; 70:661-7.
|
| [11] |
Singh A, Chatterjee S, Bansal P, Bansal A, Rawal S. Robotassisted retroperitoneal lymph node dissection: feasibility and outcome in postchemotherapy residual mass in testicular cancer. Indian J Urol 2017; 33:304-9.
|
| [12] |
Mittakanti HR, Porter JR. Robotic retroperitoneal lymph node dissection for testicular cancer: feasibility and latest outcomes. Curr Opin Urol 2019; 29:173-9.
|
| [13] |
Pearce SM, Golan S, Gorin MA, Luckenbaugh AN, Williams SB, Ward JF, et al. Safety and early oncologic effectiveness of primary robotic retroperitoneal lymph node dissection for nonseminomatous germ cell testicular cancer. Eur Urol 2017; 71:476-82.
|
| [14] |
Harris KT, Gorin MA, Ball MW, Pierorazio PM, Allaf ME. A comparative analysis of robotic vs. laparoscopic retroperitoneal lymph node dissection for testicular cancer. BJU Int 2015; 116:920-3.
|
| [15] |
Cheney SM, Andrews PE, Leibovich BC, Castle EP. Robotassisted retroperitoneal lymph node dissection: technique and initial case series of 18 patients. BJU Int 2015; 115:114-20.
|
| [16] |
Overs C, Beauval JB, Mourey L, Rischmann P, Soulié M, Roumiguié M, et al. Robot-assisted post-chemotherapy retroperitoneal lymph node dissection in germ cell tumor: is the single-docking with lateral approach relevant? World J Urol 2018; 36:655-61.
|
| [17] |
Kamel MH, Littlejohn N, Cox M, Eltahawy EA, Davis R. Postchemotherapy robotic retroperitoneal lymph node dissection: institutional experience. J Endourol 2016; 30:510-9.
|
| [18] |
Li R, Duplisea JJ, Petros FG, González GMN, Tu S-M, Karam JA, et al. Robotic postchemotherapy retroperitoneal lymph node dissection for testicular cancer. Eur Urol Oncol 2019; S2588-9311:30015-X. https://doi.org/10.1016/j.euo.2019.01.014.
|
| [19] |
Calaway AC, Einhorn LH, Masterson TA, Foster RS, Cary C. Adverse surgical outcomes associated with robotic retroperitoneal lymph node dissection among patients with testicular cancer. Eur Urol 2019; 76:607-9.
|
| [20] |
Bhayani SB, Allaf ME, Kavoussi LR. Laparoscopic RPLND for clinical stage I nonseminomatous germ cell testicular cancer: current status. Urol Oncol 2004; 22:145-8.
|
| [21] |
Schwartz MJ, Kavoussi LR. Controversial technology: the Chunnel and the laparoscopic retroperitoneal lymph node dissection (RPLND). BJU Int 2010; 106:950-9.
|
| [22] |
Abboudi H, Khan MS, Guru KA, Froghi S, de Win G, Van Poppel H, et al. Learning curves for urological procedures: a systematic review. BJU Int 2014; 114:617-29.
|
| [23] |
Torricelli FCM, Jardim D, Guglielmetti GB, Patel V, Coelho RF. Robot-assisted laparoscopic retroperitoneal lymph node dissection in testicular tumor. Int Braz J Urol 2017; 43:171. https://doi.org/10.1590/S1677-5538.IBJU.2015.0436.
pmid: 28124545
|
| [24] |
Lee SH, Kim DS, Chang S-G, Jeon SH. Robot-assisted laparoscopic retroperitoneal lymph node dissection for stage IIIb mixed germ cell testicular cancer after chemotherapy. J Urol 2015; 56:540-4.
|
| [25] |
Zhang K, Zhu G, Liu X, Tian J, Gu Y, Zhai M, et al. Robotassisted laparoscopic retroperitoneal lymph node dissection with concomitant inferior vena cava thrombectomy for metastatic mixed testicular germ cell cancer: a case report. J Med Case Rep 2019; 13:272. https://doi.org/10.1186/s13256-019-2200-y.
doi: 10.1186/s13256-019-2200-y
pmid: 31451109
|
| [26] |
Patel HD, Mullins JK, Pierorazio PM, Jayram G, Cohen JE, Matlaga BR, et al. Trends in renal surgery: robotic technology is associated with increased use of partial nephrectomy. J Urol 2013; 189:1229-35.
|
| [27] |
Pierorazio PM, Patel HD, Feng T, Yohannan J, Hyams ES, Allaf ME. Robotic-assisted versus traditional laparoscopic partial nephrectomy: comparison of outcomes and evaluation of learning curve. Urology 2011; 78:813-9.
|
| [28] |
Tamhankar AS, Patil SR, Ojha SP, Ahluwalia P, Gautam G. Therapeutic supine robotic retroperitoneal lymph node dissection for post-chemotherapy residual masses in testicular cancer: technique and outcome analysis of initial experience. J Robot Surg 2019; 13:747-56.
|
| [29] |
Stephenson AJ, Klein EA. Surgical management of low-stage nonseminomatous germ cell testicular cancer. BJU Int 2009; 104:1362-8.
|
| [30] |
Beck SD, Foster RS, Bihrle R, Ulbright T, Koch MO, Wahle GR, et al. Teratoma in the orchiectomy specimen and volume of metastasis are predictors of retroperitoneal teratoma in postchemotherapy nonseminomatous testis cancer. J Urol 2002; 168:1402-4.
|
| [31] |
Fernandez EB, Moul JW, Foley JP, Colon E, McLeod DG. Retroperitoneal imaging with third and fourth generation computed axial tomography in clinical stage I nonseminomatous germ cell tumors. Urology 1994; 44:548-52.
|
| [32] |
Subramanian VS, Nguyen CT, Stephenson AJ, Klein EA. Complications of open primary and post-chemotherapy retroperitoneal lymph node dissection for testicular cancer. Urol Oncol 2010; 28:504-9.
|
| [33] |
Albers P, Siener R, Krege S, Schmelz H-U, Dieckmann K-P, Heidenreich A, et al. Randomized phase III trial comparing retroperitoneal lymph node dissection with one course of bleomycin and etoposide plus cisplatin chemotherapy in the adjuvant treatment of clinical stage I Nonseminomatous testicular germ cell tumors: AUO trial AH 01/94 by the German Testicular Cancer Study Group. J Clin Oncol 2008; 26:2966-72.
|
| [34] |
Foss? SD, Aass N, Winderen M, B?rmer OP, Olsen DR. Longterm renal function after treatment for malignant germ-cell tumours. Ann Oncol 2002; 13:222-8.
|
| [35] |
Meinardi MT, Gietema JA, van der Graaf WT, van Veldhuisen DJ, Runne MA, Sluiter WJ, et al. Cardiovascular morbidity in long-term survivors of metastatic testicular cancer. J Clin Oncol 2000; 18:1725-32.
|
| [36] |
Huddart RA, Norman A, Shahidi M, Horwich A, Coward D, Nicholls J, et al. Cardiovascular disease as a long-term complication of treatment for testicular cancer. J Clin Oncol 2003; 21:1513-23.
|
| [37] |
Nuver J, Smit AJ, van der Meer J, van den Berg MP, van der Graaf WTA, Meinardi MT, et al. Acute chemotherapy-induced cardiovascular changes in patients with testicular cancer. J Clin Oncol 2005; 23:9130-7.
|
| [38] |
van den Belt-Dusebout AW, de Wit R, Gietema JA, Horenblas S, Louwman MWJ, Ribot JG, et al. Treatment-specific risks of second malignancies and cardiovascular disease in 5-year survivors of testicular cancer. J Clin Oncol 2007; 25:4370-8.
|
| [39] |
Bryd?y M, Foss? SD, Klepp O, Bremnes RM, Wist EA, Wentzel- Larsen T, et al. Paternity following treatment for testicular cancer. J Natl Cancer Inst 2005; 97:1580-8.
|
| [40] |
Katz MH, Eggener SE. The evolution, controversies, and potential pitfalls of modified retroperitoneal lymph node dissection templates. World J Urol 2009; 27:477-83.
|
| [41] |
Rassweiler JJ, Scheitlin W, Heidenreich A, Laguna MP, Janetschek G. Laparoscopic retroperitoneal lymph node dissection: does it still have a role in the management of clinical stage I nonseminomatous testis cancer? A European perspective. Eur Urol 2008; 54:1004-15.
|
| [42] |
Williams SB, McDermott DW, Winston D, Bahnson E, Berry AM, Steele GS, et al. Morbidity of open retroperitoneal lymph node dissection for testicular cancer: contemporary perioperative data. BJU Int 2010; 105:918-21.
|
| [43] |
Werntz RP, Pearce SM, Eggener SE. Indications, evolving technique, and early outcomes with robotic retroperitoneal lymph node dissection. Curr Opin Urol 2018; 28:461-8.
|
| [44] |
Nayan M, Jewett MAS, Sweet J, Anson-Cartwright L, Bedard PL, Moore M, et al. Lymph node yield in primary retroperitoneal lymph node dissection for nonseminoma germ cell tumors. J Urol 2015; 194:386-91.
|
| [45] |
Macleod LC, Rajanahally S, Nayak JG, Parent BA, Ramos JD, Schade GR, et al. Characterizing the morbidity of postchemotherapy retroperitoneal lymph node dissection for testis cancer in a national cohort of privately insured patients. Urology 2016; 91:70-6.
|
| [46] |
Calestroupat J-P, Sanchez-Salas R, Cathelineau X, Rozet F, Galiano M, Smyth G, et al. Postchemotherapy laparoscopic retroperitoneal lymph node dissection in nonseminomatous germ-cell tumor. J Endourol 2009; 23:645-50.
|
| [47] |
Wells H, Hayes MC, O’Brien T, Fowler S. Contemporary retroperitoneal lymph node dissection (RPLND) for testis cancer in the UKda national study. BJU Int 2017; 119:91-9.
|
| [48] |
Woldu SL, Matulay JT, Clinton TN, Singla N, Krabbe L-M, Hutchinson RC, et al. Impact of hospital case volume on testicular cancer outcomes and practice patterns. Urol Oncol 2018; 36:e7-15. https://doi.org/10.1016/j.urolonc.2017.08.024.14.
|
| [49] |
Pettus JA, Carver B, Masterson T, Stasi J, Sheinfeld J. Preservation of ejaculation in patients undergoing nervesparing post-chemotherapy retroperitoneal lymph node dissection for metastatic testicular cancer. Urology 2009; 73:328-32.
|
| [50] |
Syan-Bhanvadia S, Bazargani ST, Clifford TG, Cai J, Miranda G, Daneshmand S. Midline extraperitoneal approach to retroperitoneal lymph node dissection in testicular cancer: minimizing surgical morbidity. Eur Urol 2017; 72:814-20.
|
| [51] |
Hiester A, Nini A, Fingerhut A, Gro?e Siemer R, Winter C, Albers P, et al. Preservation of ejaculatory function after postchemotherapy retroperitoneal lymph node dissection (PCRPLND) in patients with testicular cancer: template vs. bilateral resection. Front Surg 2019; 5:80. https://doi.org/10.3389/fsurg.2018.00080.
pmid: 30705885
|
| [1] |
Gilberto José Rodrigues,Giuliano Betoni Guglielmetti,Marcelo Orvieto,Kulthe Ramesh Seetharam Bhat,Vipul R. Patel,Rafael Ferreira Coelho. Robot-assisted endoscopic inguinal lymphadenectomy: A review of current outcomes[J]. Asian Journal of Urology, 2021, 8(1): 20-26. |
| [2] |
Dean Laganosky,Christopher P. Filson,Dattatraya Patil,Viraj A. Master. Survival benefit with extended lymphadenectomy for advanced renal malignancy: A population-based analysis[J]. Asian Journal of Urology, 2020, 7(1): 29-36. |
| [3] |
Weil R. Lai, Benjamin R. Lee. Techniques to resect the distal ureter in robotic/laparoscopic nephroureterectomy[J]. Asian Journal of Urology, 2016, 3(3): 120-125. |
|
|
|
|