|
|
|
| Nerve-sparing robot-assisted radical prostatectomy: Current perspectives |
Anup Kumara,*( ),Vipul R. Patelb,Sridhar Panaiyadiyanc,Kulthe Ramesh Seetharam Bhatb,Marcio Covas Moschovasb,Brusabhanu Nayakc ),Vipul R. Patelb,Sridhar Panaiyadiyanc,Kulthe Ramesh Seetharam Bhatb,Marcio Covas Moschovasb,Brusabhanu Nayakc
|
a Department of Urology,Robotics and Renal Transplant, Vardhman Mahaveer Medical College and Safdarjang Hospital, New Delhi, India
b Department of Robotic Surgery, AdventHealth Global Robotics Institute, Celebration, FL, USA
c Department of Urology, All India Institute of Medical Sciences, New Delhi, India |
|
|
|
|
Abstract Robotic-assisted radical prostatectomy (RARP) is the current standard of care with long term cure in organ-confined disease. The introduction of nerve-sparing (NS) to standard RARP has shown positive results in terms of functional outcomes in addition to the oncological outcomes. This article reviews the current perspectives of NS-RARP in terms of applied anatomy of the prostatic fascial planes, the neurovascular bundle (NVB), various NS techniques and postoperative functional outcomes. A non-systematic review was done using PubMed, Embase and Medline databases to retrieve and analyse articles in English, with following keywords “prostate cancer”, “robotic radical prostatectomy”, “nerve-sparing”. The Delphi method was used with an expert panel of robotic surgeons in urology to analyse the potency outcomes of various published comparative and non-comparative studies. The literature has shown that NS-RARP involves various techniques and approaches while there is a lack of randomized studies to suggest the superiority of one over the other. Variables such as preoperative risk assessments, baseline potency, surgical anatomy of individual patients and surgeons’ expertise play a major role in the outcomes. A tailored approach for each patient is required for applying the NS approach during RARP.
|
|
Received: 23 December 2019
Available online: 20 January 2021
|
|
Corresponding Authors:
Anup Kumar
E-mail: anup_14k@yahoo.com
|
|
|
|
|
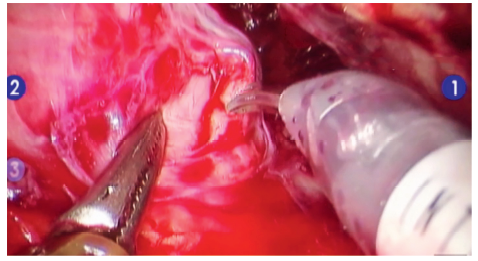
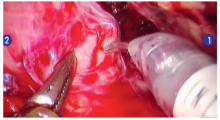
Landmark artery on anterolateral aspect of prostate.
|
|
|
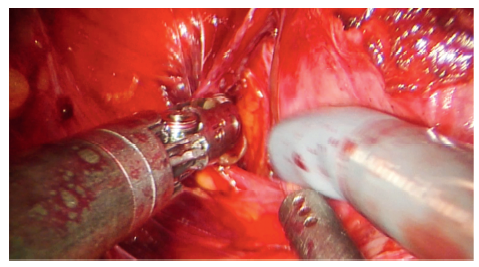
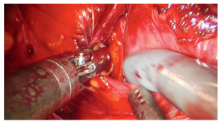
Left retrograde dissection towards the base of the prostate to completely detach the NVB from the prostatic pedicle. NVB, neurovascular bundle.
|

| Grade | Percentage of NS | Description | | Grade 5 | Complete NS (≥95% NS) | After LA is identified and NVB delineated, the NS is performed medial to LA between the prostate and the NVB. The correct plane is confirmed by the pink colour of the prostate. | | Grade 4 | Near-complete NS (75%) | After LA is identified, NS is completed by a sharp dissection between LA and the prostate capsule across the NVB and the correct planed is confirmed by the strip of fat over the prostate. | | Grade 3 | Partial NS (50%) | After LA identification, NS is performed by developing a plane lateral to the LA. The correct plane of dissection is denoted by the identification of fat strip over the prostate. | | Grade 2 | <50% NS | Herein, the NS is performed several millimeters lateral to the LA. | | Grade 1 | Non-NS (0% NS) | Herein, wide resection of the NVB is performed. The correct plane of dissection is denoted by the presence of levator fascia which is not incised. |
|
|
Anatomic grading of the proportion of nerve-sparing.
|
|
|
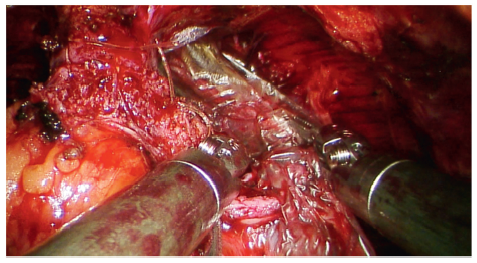
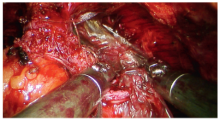
dHAM placed over as right sided nerve wrap on NVB. dHACM, dehydrated human amnion/chorion membrane; NVB, neurovascular bundles.
|
|
|
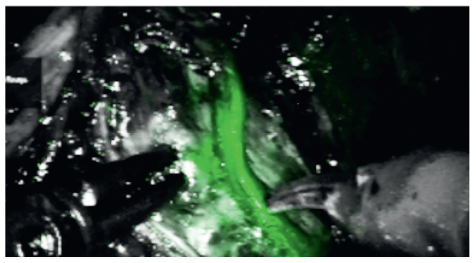
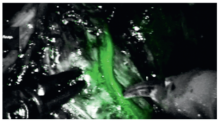
Landmark artery seen as green fluorescent structure over lateral surface of prostate in near infrared fluorescence mode.
|
| Year of the study | Author | Number of patients | Mean age (year) | NS technique | Definition of potency | Follow-up (month) | Potency rate (unilateral NS) | Potency rate (bilateral NS) | Potency rate (overall) | | 2007 | Menon et al. [14] | 721 | 60.2 | Antegrade | Adequate erection for intercourse±PDE 5 inhibitors | 12 | - | 79.2% | 79.2% | | 2009 | Potdevin et al. [8] | 147 | 58.5 vs. 58.7 | Retrograde (Interfascial-77 vs. intrafascial-70) | Adequate erection for intercourse±PDE 5 inhibitors | 9 | - | - | 3 months-16.67% vs. 24.24%
6 months-43.75% vs. 81.81%
9 months-66.67% vs. 90.9% | | 2009 | Shikanov et al. [9] | 813 | 60 vs. 58.5 | Antegrade (Extrafascial-110 vs. interfascial- 703) | Adequate erection for intercourse±PDE 5 inhibitors | 8 vs. 13 | - | - | 3 months-22% vs. 42%
6 months-34% vs. 47%
12 months-40% vs. 64% | | 2010 | Patel et al. [47] | 404 | 58 | Retrograde | Adequate erection for intercourse in >50% of attempts±PDE 5 inhibitors | 18 | - | 53.5%-6 weeks
68.8%-3 months
91.5%-6 months
97.4%-12 months
96.6%-18 months | - | | 2011 | Patel et al. [46] | 332 | 58.5 | Retrograde | Adequate erection for intercourse in >50% of attempts±PDE 5 inhibitors | 12 (minimum) | - | 53.9%-6 weeks
68%-3 months
86.1%-6 months
89.8%-1 year | - | | 2011 | Kowalczyk et al. [45] | 342-NS-0C vs.
268-NS-C | 59.6 vs. 57.9 | Antegrade | Adequate erection for intercourse±PDE 5 inhibitors | 12 | - | 5 months-45% vs. 28.4%
12 months-50% vs. 54.1% | - | | 2012 | Alemozaffar et al. [48] | 400 | 59.8 | Retrograde | Adequate erection for intercourse±PDE 5 inhibitors | 12 | - | - | 5 months-33.3%
12 months-59.3% | | 2013 | Ko et al. [18] | 344 | 57.9 vs. 57.2 | Antegrade NS-172 vs.
Retrograde NS-172 | Adequate erection for intercourse in >50% of attempts±PDE 5 inhibitors | 12 (minimum) | - | 3 months-65% vs. 80.8%
6 months-72.1% vs. 90.1%
9 months-85.3% vs. 92.9% | - | | 2013 | Ficarra et al. [2] | 183 | 62.3 | Antegrade | Adequate erection for intercourse±PDE 5 inhibitors | 81.3 | - | - | 10%-3 months
53%-6 months
82%-12 months |
|
|
Various non comparative studies reporting potency outcomes in patients undergoing robot-assisted radical prostatectomy.
|
| Year | Author | Study design | Number of patients (n) | Mean age (year) | Follow-up (month) | Inclusion criteria | Definition of potency | NS technique | Potency rate (unilateral NS) | Potency rate (bilateral NS) | Potency rate (overall) | | 2009 | Krambeck et al. [51] | RRP vs. RARP: Matched cohort analysis | 588 vs. 294 | 61 vs. 65 | 12 | All patients | Adequate erection for intercourse in last 4 weeks ± PDE 5 inhibitors | Antegrade | | | 62.8% vs. 70% | | 2009 | Rocco et al. [50] | RRP vs. RARP:
Matched cohort analysis | 105 vs. 103 | 63 vs. 63 | 12 | All patients | Adequate erection for intercourse in last 4 weeks ± PDE 5 inhibitors | Retrograde | - | - | 41% vs. 61% | | 2009 | Ficarra et al. [49] | RRP vs. RARP: Non randomised prospective study | 588 vs. 294 | 61 vs. 65 | 12 | Consecutive patients with bilateral NS | 11 EF >17 | Antegrade | - | 49% vs. 81% | |
|
|
Studies comparing outcomes between RARP vs. RRP.
|
| Year | Author | Study design | Number of patients (n) | Mean age (year) | Follow-up (month) | Inclusion criteria | Definition of potency | Nerve-sparing technique | Potency rate (unilateral NS) | Potency rate (bilateral NS) | Potency rate (overall) | | 2012 | Willis et al. [58] | RARP vs. LRP | 174 vs. 175 | 58.1 vs. 58.2 | 12 | Consecutive patients with localized prostate cancer | Adequate erection for intercourse in last 4 weeks±PDE 5 inhibitors | Antegrade | - | - | 3 months-59.8% vs. 42.2%
6 months-71.2% vs. 51.3%
12 months-73.7% vs. 66.2% | | 2013 | Berge et al. [53] | LRP vs. RARP | 210 vs. 210 | 61.7 vs. 61.7 | 36 | Consecutive patients with localized prostate cancer | Adequate erection for intercourse±PDE 5 inhibitors | Antegrade | 40.2% vs. 45.9% (at 36 months) | 57.3% vs. 61.3% (at 36 months) | - | | 2013 | Porpiglia et al. [54] | RARP vs. LRP (RCT) | 60 vs. 60 | 63.9 vs. 64.7 | 12 | Consecutive patients with localized prostate cancer | IIEF-5 score >17 | Antegrade | - | - | 80% vs. 54.2% (12 months) | | 2013 | Asimakopoulos et al. [55] | LRP vs. RARP | 91 vs. 136 | 63 vs. 60 | 18 vs. 21 | Age ≤70 years, clinically localized prostate cancer, preoperativepotent, with bilateral NS | Adequate erection for intercourse in last 4 weeks ± PDE 5 inhibitors | Antegrade | - | - | 66.2% vs. 39.6% |
|
|
Studies comparing outcomes between robot-assisted RARP vs. LRP.
|
| [1] |
Ferlay J, Soerjomataram I, Dikshit R, Eser S, Mathers C, Rebelo M, et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Canc 2015; 136:E359-86. https://doi.org/10.1002/ijc.29210.
|
| [2] |
Ficarra V, Borghesi M, Suardi N, De Naeyer G, Novara G, Schatteman P, et al. Long-term evaluation of survival, continence and potency (SCP) outcomes after robot-assisted radical prostatectomy (RARP). BJU Int 2013; 112:338-45.
|
| [3] |
Eastham JA, Scardino PT, Kattan MW. Predicting an optimal outcome after radical prostatectomy: the trifecta nomogram. J Urol 2008; 179:2207-11.
|
| [4] |
Esper P, Mo F, Chodak G, Sinner M, Cella D, Pienta KJ. Measuring quality of life in men with prostate cancer using the functional assessment of cancer therapy-prostate instrument. Urology 1997; 50:920-8.
|
| [5] |
Sooriakumaran P, Haendler L, Nyberg T, Gronberg H, Nilsson A, Carlsson S, et al. Biochemical recurrence after robot-assisted radical prostatectomy in a European single-centre cohort with a minimum follow-up time of 5 years. Eur Urol 2012; 62:768-74.
|
| [6] |
Walsh PC, Donker PJ. Impotencefollowing radical prostatectomy: insight into etiology and prevention. J Urol 1982; 128:492-7.
|
| [7] |
Tavuk?u HH, Aytac O, Atug F. Nerve-sparing techniques and results in robot-assisted radical prostatectomy. Invest Clin Urol 2016;57:S172. https://doi.org/10.4111/icu.2016.57.S2.S172.
|
| [8] |
Potdevin L, Ercolani M, Jeong J, Kim IY. Functional and oncologic outcomes comparing interfascial and intrafascial nerve sparing in robot-assisted laparoscopic radical prostatectomies. J Endourol 2009; 23:1479-84.
|
| [9] |
Shikanov S, Woo J, Al-Ahmadie H, Katz MH, Zagaja GP, Shalhav AL, et al. Extrafascial versus interfascial nervesparing technique for robotic-assisted laparoscopic prostatectomy: comparison of functional outcomes and positive surgical margins characteristics. Urology 2009; 74:611-6.
|
| [10] |
Tewari A, Takenaka A, Mtui E, Horninger W, Peschel R, Bartsch G, et al. The proximal neurovascular plate and the trizonal neural architecture around the prostate gland: importance in the athermal robotic technique of nerve-sparing prostatectomy. BJU Int 2006; 98:314-23.
|
| [11] |
Stolzenburg JU, Rabenalt R, Do M, Schwalenberg T, Winkler M, Dietel A, et al. Intrafascial nerve-sparing endoscopic extraperitoneal radical prostatectomy. Eur Urol 2008; 53:931-40.
|
| [12] |
Martinez-Salamanca JI, Ramanathan R, Rao S, Mandhani A, Leung R, Horninger W, et al. Second Prize: pelvic neuroanatomy and innovative approaches to minimize nerve damage and maximize cancer control in patients undergoing robot-assisted radical prostatectomy. J Endourol 2008; 22:1137-46.
|
| [13] |
Carter S, Le JD, Hu JC. Anatomic and technical considerations for optimizing recovery of sexual function during roboticassisted radical prostatectomy. Curr Opin Urol 2013; 23:88-94.
|
| [14] |
Menon M, Shrivastava A, Kaul S, Badani KK, Fumo M, Bhandari M, et al. Vattikuti Institute prostatectomy: contemporary technique and analysis of results. Eur Urol 2007; 51:648-58.
|
| [15] |
Ficarra V, Novara G, Artibani W, Cestari A, Galfano A, Graefen M, et al. Retropubic, laparoscopic, and robot-assisted radical prostatectomy: a systematic review and cumulative analysis of comparative studies. Eur Urol 2009; 55:1037-63.
|
| [16] |
Ahlering TE, Eichel L, Chou D, Skarecky DW. Feasibility study for robotic radical prostatectomy cautery-free neurovascular bundle preservation. Urology 2005; 65:994-7.
|
| [17] |
Walz J, Burnett AL, Costello AJ, Eastham JA, Graefen M, Guillonneau B, et al. A critical analysis of the current knowledge of surgical anatomy related to optimization of cancer control and preservation of continence and erection in candidates for radical prostatectomy. Eur Urol 2010; 57:179-92.
|
| [18] |
Ko YH, Coelho RF, Sivaraman A, Schatloff O, Chauhan S, Abdul-Muhsin HM, et al. Retrograde versus antegrade nerve sparing during robot-assisted radical prostatectomy: which is better for achieving early functional recovery? Eur Urol 2013; 63:169-77.
|
| [19] |
Kaul S, Savera A, Badani K, Fumo M, Bhandari A, Menon M. Functional outcomes and oncological efficacy of Vattikuti Institute prostatectomy with Veil of Aphrodite nervesparing: an analysis of 154 consecutive patients. BJU Int 2006; 97:467-72.
|
| [20] |
Menon M, Shrivastava A, Bhandari M, Satyanarayana R, Siva S, Agarwal PK. Vattikuti Institute prostatectomy: technical modifications in 2009. Eur Urol 2009; 56:89-96.
|
| [21] |
Ghani KR, Trinh QD, Menon M. Vattikuti institute prostatectomy-technique in 2012. J Endourol 2012; 26:1558-65.
|
| [22] |
Patel VR, Schatloff O, Chauhan S, Sivaraman A, Valero R, Coelho RF, et al. The role of the prostatic vasculature as a landmark for nerve sparing during robot-assisted radical prostatectomy. Eur Urol 2012; 61:571-6.
|
| [23] |
Finley DS, Osann K, Skarecky D, Ahlering TE. Hypothermic nerve-sparing radical prostatectomy: rationale, feasibility, and effect on early continence. Urology 2009; 73:691-6.
|
| [24] |
Chien GW, Mikhail AA, Orvieto MA, Zagaja GP, Sokoloff MH, Brendler CB, et al. Modified clipless antegrade nerve preservation in robotic-assisted laparoscopic radical prostatectomy with validated sexual function evaluation. Urology 2005; 66:419-23.
|
| [25] |
Schatloff O, Chauhan S, Sivaraman A, Kameh D, Palmer KJ, Patel VR. Anatomic grading of nerve sparing during robotassisted radical prostatectomy. Eur Urol 2012; 61:796-802.
|
| [26] |
Schatloff O, Chauhan S, Kameh D, Valero R, Ko YH, Sivaraman A, et al. Cavernosal nerve preservation during robot-assisted radical prostatectomy is a graded rather than an all-or-none phenomenon: objective demonstration by assessment of residual nerve tissue on surgical specimens. Urology 2012; 79:596-600.
|
| [27] |
Cheetham PJ, Truesdale MD, Lee DJ, Landman JM, Badani KK. Use of a flexible carbon dioxide laser fiber for precise dissection of the neurovascular bundle during robot-assisted laparoscopic prostatectomy. J Endourol 2010; 24:1091-6.
|
| [28] |
Kumar A, Samavedi S, Bates A, Coelho R, Rocco B, Marquinez J, et al. Using indocyanine green and near-infrared fluorescence technology to identify the “landmark artery” during robot-assisted radical prostatectomy. Videourology 2015; 29. https://doi.org/10.1089/vid.2014.0071.vid.2014.0071.
pmid: 32292640
|
| [29] |
Schlomm T, Tennstedt P, Huxhold C, Steuber T, Salomon G, Michl U, et al. Neurovascular structure-adjacent frozen-section examination (NeuroSAFE) increases nerve-sparing frequency and reduces positive surgical margins in open and robot-assisted laparoscopic radical prostatectomy: experience after 11,069 consecutive patients. Eur Urol 2012; 62:333-40.
|
| [30] |
Puliatti S, Bertoni L, Pirola GM, Azzoni P, Bevilacqua L, Eissa A, et al. Ex vivo fluorescence confocal microscopy: the first application for real-time pathological examination of prostatic tissue. BJU Int 2019; 124:469-76.
|
| [31] |
Bertoni L, Puliatti S, Reggiani Bonetti L, Maiorana A, Eissa A, Azzoni P, et al. Ex vivo fluorescence confocal microscopy: prostatic and periprostatic tissues atlas and evaluation of the learning curve. Virchows Arch 2020; 476:511-20.
|
| [32] |
Schiavina R, Bianchi L, Borghesi M, Dababneh H, Chessa F, Pultrone CV, et al. MRI displays the prostatic cancer anatomy and improves the bundles management before robot-assisted radical prostatectomy. J Endourol 2018; 32:315-21.
|
| [33] |
Kozikowski M, Malewski W, Michalak W, Dobruch J. Clinical utility of MRI in the decision-making process before radical prostatectomy: systematic review and meta-analysis. PloS One 2019; 14:e0210194. https://doi.org/10.1371/journal.pone.0210194. .
pmid: 30615661
|
| [34] |
Tewari A, Srivastava A, Sooriakumaran P, Grover S, Dorsey P, Leung R. Technique of traction-free nerve-sparing robotic prostatectomy: delicate tissue handling by real-time penile oxygen monitoring. Int J Impot Res 2012; 24:11-9.
|
| [35] |
Geuna S, Muratori L, Fregnan F, Manfredi M, Bertolo R, Porpiglia F. Strategies to improve nerve regeneration after radical prostatectomy: a narrative review. Minerva Urol Nefrol 2018; 70:546-58.
|
| [36] |
Patel VR, Samavedi S, Bates AS, Kumar A, Coelho R, Rocco B, et al. Dehydrated human amnion/chorion membrane allograft nerve wrap around the prostatic neurovascular bundle accelerates early return to continence and potency following robot-assisted radical prostatectomy: propensity scorematched analysis. Eur Urol 2015; 67:977-80.
|
| [37] |
Ogaya-Pinies G, Palayapalam-Ganapathi H, Rogers T, Hernandez- Cardona E, Rocco B, Coelho RF, et al. Can dehydrated human amnion/chorion membrane accelerate the return to potency after a nerve-sparing robotic-assisted radical prostatectomy? Propensity score-matched analysis. J Robot Surg 2018; 12:235-43.
|
| [38] |
Porpiglia F, Manfredi M, Checcucci E, Garrou D, De Cillis S, Amparore D, et al. Use of chitosan membranes after nervesparing radical prostatectomy improves early recovery of sexual potency: results of a comparative study. BJU Int 2019; 123:465-73.
|
| [39] |
Porpiglia F, Fiori C, Checcucci E, Amparore D, Bertolo R. Augmented reality robot-assisted radical prostatectomy: preliminary experience. Urology 2018; 115:184. https://doi.org/10.1016/j.urology.2018.01.028.
pmid: 29548868
|
| [40] |
Porpiglia F, Bertolo R, Amparore D, Checcucci E, Artibani W, Dasgupta P, et al. Augmented reality during robot-assisted radical prostatectomy: expert robotic surgeons’ on-the-spot insights after live surgery. Minerva Urol Nefrol 2018; 70:226-9.
|
| [41] |
Porpiglia F, Checcucci E, Amparore D, Autorino R, Piana A, Bellin A, et al. Augmented-reality robot-assisted radical prostatectomy using hyper-accuracy three-dimensional reconstruction (HA3DTM) technology: a radiological and pathological study. BJU Int 2019; 123:834-45.
|
| [42] |
Finley DS, Rodriguez E, Skarecky DW, Ahlering TE. Quantitative and qualitative analysis of the recovery of potency after radical prostatectomy: effect of unilateral vs. bilateral nerve sparing. BJU Int 2009; 104:1484-9.
|
| [43] |
Greco F, Hoda MR, Wagner S, Reichelt O, Inferrera A, Magno C, et al. Bilateral vs. unilateral laparoscopic intrafascial nervesparing radical prostatectomy: evaluation of surgical and functional outcomes in 457 patients. BJU Int 2011; 108:583-7.
|
| [44] |
Avulova S, Zhao Z, Lee D, Huang LC, Koyama T, Hoffman KE, et al. The effect of nerve sparing status on sexual and urinary function: 3-year results from the CEASAR study. J Urol 2018; 199:1202-9.
|
| [45] |
Kowalczyk KJ, Huang AC, Hevelone ND, Lipsitz SR, Yu H, Ulmer WD, et al. Stepwise approach for nerve sparing without countertraction during robot-assisted radical prostatectomy: technique and outcomes. Eur Urol 2011; 60:536-47.
|
| [46] |
Patel VR, Sivaraman A, Coelho RF, Chauhan S, Palmer KJ, Orvieto MA, et al. Pentafecta: a new concept for reporting outcomes of robot-assisted laparoscopic radical prostatectomy. Eur Urol 2011; 59:702-7.
|
| [47] |
Patel VR, Coelho RF, Chauhan S, Orvieto MA, Palmer KJ, Rocco B, et al. Continence, potency and oncological outcomes after robotic-assisted radical prostatectomy: early trifecta results of a high-volume surgeon. BJU Int 2010; 106:696-702.
|
| [48] |
Alemozaffar M, Duclos A, Hevelone ND, Lipsitz SR, Borza T, Yu HY, et al. Technical refinement and learning curve for attenuating neurapraxia during robotic-assisted radical prostatectomy to improve sexual function. Eur Urol 2012; 61:1222-8.
|
| [49] |
Ficarra V, Novara G, Fracalanza S, D’Elia C, Secco S, Iafrate M, et al. A prospective, non-randomized trial comparing robotassisted laparoscopic and retropubic radical prostatectomy in one European institution. BJU Int 2009; 104:534-9.
|
| [50] |
Rocco B, Matei DV, Melegari S, Ospina JC, Mazzoleni F, Errico G, et al. Robotic vs. open prostatectomy in a laparoscopically naive centre: a matched-pair analysis. BJU Int 2009; 104:991-5.
|
| [51] |
Krambeck AE, DiMarco DS, Rangel LJ, Bergstralh EJ, Myers RP, Blute ML, et al. Radical prostatectomy for prostatic adenocarcinoma: a matched comparison of open retropubic and robot-assisted techniques. BJU Int 2009; 103:448-53.
|
| [52] |
Haese A, Knipper S, Isbarn H, Heinzer H, Tilki D, Salomon G, et al. A comparative study of robot-assisted and open radical prostatectomy in 10 790 men treated by highly trained surgeons for both procedures. BJU Int 2019; 123:1031-40.
|
| [53] |
Berge V, Berg RE, Hoff JR, Wessel N, Diep LM, Karlsen SJ, et al. A prospective study of transition from laparoscopic to robotassisted radical prostatectomy: quality of life outcomes after 36-month follow-up. Urology 2013; 81:781-6.
|
| [54] |
Porpiglia F, Morra I, Lucci Chiarissi M, Manfredi M, Mele F, Grande S, et al. Randomised controlled trial comparing laparoscopic and robot-assisted radical prostatectomy. Eur Urol 2013; 63:606-14.
|
| [55] |
Asimakopoulos AD, Miano R, Di Lorenzo N, Spera E, Vespasiani G, Mugnier C. Laparoscopic versus robot-assisted bilateral nerve-sparing radical prostatectomy: comparison of pentafecta rates for a single surgeon. Surg Endosc 2013; 27:4297-304.
|
| [56] |
Ou YC, Yang CK, Kang HM, Chang KS, Wang J, Hung SW, et al. Pentafecta outcomes of 230 cases of robotic-assisted radical prostatectomy with bilateral neurovascular bundle preservation. Anticancer Res 2015; 35:5007-13.
|
| [57] |
Jazayeri SB, Weissman B, Samadi DB. Outcomes following robotic-assisted laparoscopic prostatectomy: pentafecta and Trifecta achievements. Minerva Urol Nefrol 2018; 70:66-73.
|
| [58] |
Willis DL, Gonzalgo ML, Brotzman M, Feng Z, Trock B, Su LM. Comparison of outcomes between pure laparoscopic vs. robotassisted laparoscopic radical prostatectomy: a study of comparative effectiveness based upon validated quality of life outcomes. BJU Int 2012; 109:898-905.
|
| [1] |
Wattanachai Ratanapornsompong,Suthep Pacharatakul,Premsant Sangkum,Chareon Leenanupan,Wisoot Kongcharoensombat. Effect of puboprostatic ligament preservation during robotic-assisted laparoscopic radical prostatectomy on early continence: Randomized controlled trial[J]. Asian Journal of Urology, 2021, 8(3): 260-268. |
| [2] |
Kevin J. Hebert,Brian J. Linder,Griffin T. Morrisson,Laureano Rangel Latuche,Daniel S. Elliott. A comparison of artificial urinary sphincter outcomes after primary implantation and first revision surgery[J]. Asian Journal of Urology, 2021, 8(3): 298-302. |
| [3] |
Mengzhu Liu,Kun Jin,Shi Qiu,Pengyong Xu,Mingming Zhang,Wufeng Cai,Xiaonan Zheng,Lu Yang,Qiang Wei. Oncological outcomes of patients with ductal adenocarcinoma of the prostate receiving radical prostatectomy or radiotherapy[J]. Asian Journal of Urology, 2021, 8(2): 227-234. |
| [4] |
Fubo Wang,Chao Zhang,Fei Guo,Xia Sheng,Jin Ji,Yalong Xu,Zhi Cao,Ji Lyu,Xiaoying Lu,Bo Yang. The application of virtual reality training for anastomosis during robot-assisted radical prostatectomy[J]. Asian Journal of Urology, 2021, 8(2): 204-208. |
| [5] |
Zepeng Jia,Yifan Chang,Yan Wang,Jing Li,Min Qu,Feng Zhu,Huan Chen,Bijun Lian,Meimian Hua,Yinghao Sun,Xu Gao. Sustainable functional urethral reconstruction: Maximizing early continence recovery in robotic-assisted radical prostatectomy[J]. Asian Journal of Urology, 2021, 8(1): 126-133. |
| [6] |
Marcio Covas Moschovas,Frederico Timóteo,Leonardo Lins,Oséas de Castro Neves,Kulthe Ramesh Seetharam Bhat,Vipul R. Patel. Robotic surgery techniques to approach benign prostatic hyperplasia disease: A comprehensive literature review and the state of art[J]. Asian Journal of Urology, 2021, 8(1): 81-88. |
| [7] |
Anne Holck Storås,Martin G. Sanda,Olatz Garin,Peter Chang,Dattatraya Patil,Catrina Crociani,Jose Francisco Suarez,Milada Cvancarova,Jon Håvard Loge,Sophie D. Fosså. A prospective study of patient reported urinary incontinence among American, Norwegian and Spanish men 1 year after prostatectomy[J]. Asian Journal of Urology, 2020, 7(2): 161-169. |
| [8] |
Huan Chen,Bijun Lian,Zhenyang Dong,Yan Wang,Min Qu,Feng Zhu,Yinghao Sun,Xu Gao. Experience of one single surgeon with the first 500 robot-assisted laparoscopic prostatectomy cases in mainland China[J]. Asian Journal of Urology, 2020, 7(2): 170-176. |
| [9] |
Nicolas Turmel,Samer Sheikh Ismael,Camille Chesnel,Audrey Charlanes,Claire Hentzen,Frédérique Le Breton,Gérard Amarenco. Use of a specific questionnaire and perineal electromyography to assess neuropathic pain after radical retropubic prostatectomy[J]. Asian Journal of Urology, 2019, 6(4): 364-367. |
| [10] |
Kerri Beckmann,Michael O’Callaghan,Andrew Vincent,Penelope Cohen,Martin Borg,David Roder,Sue Evans,Jeremy Millar,Kim Moretti. Extent and predictors of grade upgrading and downgrading in an Australian cohort according to the new prostate cancer grade groupings[J]. Asian Journal of Urology, 2019, 6(4): 321-329. |
| [11] |
Edwin Jonathan Aslim,Yan Mee Law,Puay Hoon Tan,John Carson Allen Jr,Lionel Tim-Ee Cheng,Viswanath Anand Chidambaram,Li Yan Khor,Benjamin Yongcheng Tan,Ernest Wencong Eu,Christopher Wai Sam Cheng,John Shyi Peng Yuen,Henry Sun Sien Ho,Lui Shiong Lee. Multiparametric MRI reporting using Prostate Imaging Reporting and Data System version 2.0 (PI-RADSv2) retains clinical efficacy in a predominantly post-biopsy patient population[J]. Asian Journal of Urology, 2019, 6(3): 256-263. |
| [12] |
Hendrik van Poppel,Wouter Everaerts,Lorenzo Tosco,Steven Joniau. Open and robotic radical prostatectomy[J]. Asian Journal of Urology, 2019, 6(2): 125-128. |
| [13] |
Najib Isse Dirie,Gaurab Pokhrel,Wei Guan,Mukhtar Adan Mumin,Jun Yang,Jackson Ferdinand Masau,Hu Henglong,Shaogang Wang. Is Retzius-sparing robot-assisted radical prostatectomy associated with better functional and oncological outcomes? Literature review and meta-analysis[J]. Asian Journal of Urology, 2019, 6(2): 174-182. |
| [14] |
Shulian Chen,Rang Gao,Hong Li,Kunjie Wang. Management of acquired rectourethral fistulas in adults[J]. Asian Journal of Urology, 2018, 5(3): 149-154. |
| [15] |
Chen Kenneth,Sim Allen,Kan Alex Ford. The effect of adjunct caudal block on postoperative analgesia in robot-assisted laparoscopic radical prostatectomy: A prospective randomized controlled, single blinded pilot study in a tertiary centre[J]. Asian Journal of Urology, 2018, 5(2): 122-126. |
|
|
|
|