|
|
|
| Laparoscopic transvesical vesicovaginal fistula repair with the least invasive way: Only three trocars and a limited posterior cystotomy |
Stilianos Giannakopoulosa,b,*( ),Halil Arifa,Zisis Nastosa,Apostolos Liapisa,Christos Kalaitzisa,Stavros Touloupidisa ),Halil Arifa,Zisis Nastosa,Apostolos Liapisa,Christos Kalaitzisa,Stavros Touloupidisa
|
aDepartment of Urology, Democritus University of Thrace, Alexandroupolis, Greece
bEndoscopy Unit, Democritus University of Thrace, Alexandroupolis, Greece |
|
|
|
|
Abstract Objective: Two conventional approaches for vesicovaginal fistula (VVF) repair are transabdominal repair for supratrigonal VVF and transvaginal approach for low lying fistulae. Laparoscopic surgery was introduced to duplicate the surgical steps of the transabdominal approach with reduction in morbidity. We report a series of patients treated with a modified laparoscopic technique which includes the use of only three trocars and a limited posterior cystotomy.
Methods: We retrospectively reviewed the data of eight patients who underwent laparoscopic VVF repair with our standardized technique from January 2015 to April 2018. Only cases with a supratrigonal fistula were included. We constantly used only three trocars. A limited 2 cm midline posterior cystotomy was performed using ultrasonic energy. A stay suture on a straight needle was passed percutaneously in the abdomen, then on either side of the cystotomy and finally was exteriorized to maintain countertraction. The cystotomy was extended downwards to include the fistula site. The fistula was dissected circumferentially to raise the bladder and vaginal flaps. The vaginal defect was closed in a transverse fashion and the cystotomy was closed vertically.
Results: Mean operative time was 178±31.6 min and estimated blood loss was 60±18.7 mL. Flap interposition was performed in six cases. No intraoperative complications were recorded. Mean hospital stay was 2.25±0.89 days. During hospitalization two patients experienced postoperative complications (Clavien grade I). Mean follow-up was 20.9±11.1 months (6.0-39.0 months). All patients remained continent during the follow-up period. Conclusions: This minimally invasive laparoscopic approach with only three trocars and limited posterior cystotomy provides excellent results with minimum morbidity.
|
|
Received: 03 December 2018
Available online: 08 July 2019
|
|
Corresponding Authors:
Stilianos Giannakopoulos
E-mail: stgian@otenet.gr
|
|
|

| Characteristic | Value | | Age, mean±SD, year | 49±8.5 | | BMI (kg/m2), n (%) | | Underweight (<18.50) | 0 (0) | | Normal range (18.50-24.99) | 3 (37.5) | | Overweight (25.00-29.99) | 4 (50) | | Obese (≥30) | 1 (12.5) | | Etiology, n (%) | | Abdominal hysterectomy | 5 (62.5) | | Laparoscopic hysterectomy | 2 (25) | | Transvaginal hysterectomy | 1 (12.5) | | Size of fistula, mean (range), mm | 6.6 (3-15) | | Fistula type, n (%) | | Primary | 7 (87.5) | | Recurrent | 1 (12.5) | | Fistula site, n (%) | | Supratrigonal | 8 (100) | | Trigonal | 0 (0) | | Infratrigonal | 0 (0) | | Interval between gynecologic injury and VVF surgery, mean (range),a month | 3.25 (2-6) |
|
|
Demographic and clinical data.
|
|
|
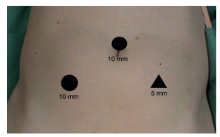
Port configuration.
|
|
|
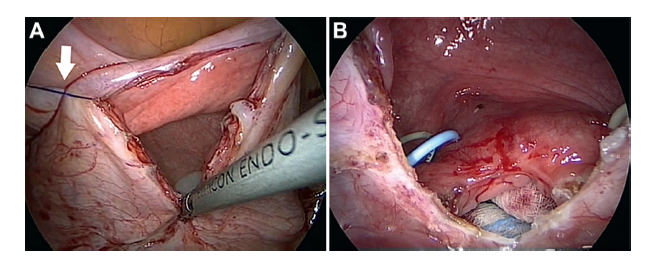
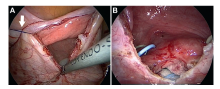
Limited posterior cystotomy. (A) Note the stay suture on either side of the cystotomy that was exteriorized to maintain countertraction (white arrow); (B) Cystotomy is extended downwards to include the fistula site.
|
|
|
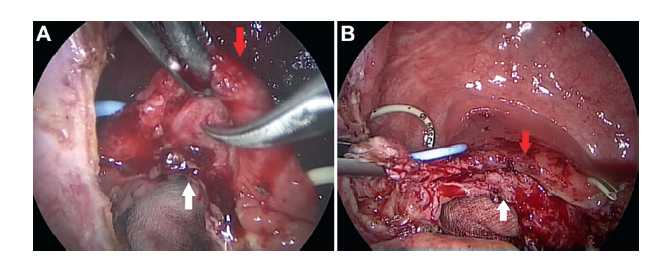
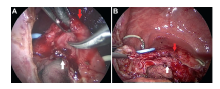
Dissection of the fistulous tract. (A) Using scissors the bladder wall (red arrow) is dissected off the vaginal wall (white arrow) circumferentially around the fistula site; (B) Complete separation of the posterior bladder wall (red arrow) from the anterior vaginal wall (white arrow).
|
|
|
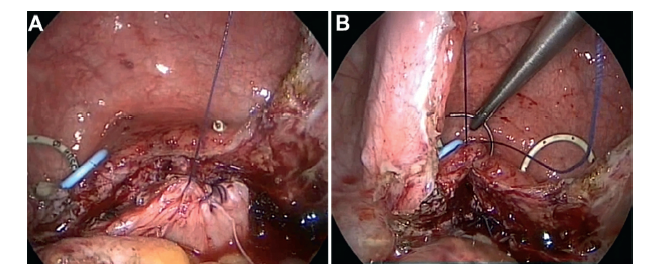
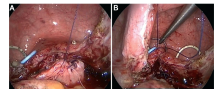
Closure of the defects. (A) The vaginal defect is closed with a running suture in a transverse fashion; (B) The cystotomy is closed vertically with a running suture in a single layer.
|
| Factor | Value | | Operative time, mean±SD, min | 178±31.6 | | Blood loss, mean±SD, mL | 60±18.7 | | Flap interposition, n (%) | | Omentum | 3 (37.5) | | Sigmoid epiploicae | 3 (37.5) | | Nothing | 2 (25) | | Hospital stay, mean±SD, day | 2.25±0.89 | | Complications, n (%) | | Clavien grade I | 2 (25) | | Clavien grade II-V | 0 (0) | | Duration of bladder catheterization, mean±SD, week | 3.37±0.7 | | Duration of stents in situ, mean±SD, week | 4.4±0.7 | | Follow-up, mean±SD, month | 20.9±11.1 | | Success, n (%) | 8 (100) |
|
|
Intraoperative and postoperative results.
|
| [1] |
Tebeu PM, Fomulu JN, Khaddaj S, de Bernis L, Delvaux T, Rochat CH. Risk factors for obstetric fistula: a clinical review. Int Urogynecol J 2012; 23:387-94.
pmid: 22143450
|
| [2] |
Harris WJ. Early complications of abdominal and vaginal hysterectomy. Obstet Gynecol Surv 1995; 50:795-805.
pmid: 8545085
|
| [3] |
Tenggardjaja CF, Goldman HB. Advances in minimally invasive repair of vesicovaginal fistulas. Curr Urol Rep 2013; 14:253-61.
pmid: 23475747
|
| [4] |
Matei DV, Zanagnolo V, Vartolomei MD, Crisan N, Ferro M, Bocciolone L, et al. Robot-assisted vesico-vaginal fistula repair: our technique and review of the literature. Urol Int 2017; 99:137-42.
doi: 10.1159/000475887
pmid: 28743109
|
| [5] |
Bora GS, Singh S, Mavuduru RS, Devana SK, Kumar S, Mete UK, et al. Robot-assisted vesicovaginal fistula repair: a safe and feasible technique. Int Urogynecol J 2017; 28:957-62.
pmid: 27844120
|
| [6] |
Nezhat CH, Nezhat F, Nezhat C. Laparoscopic repair of a vesicovaginal fistula: a case report. Obstet Gynecol 1994; 83:899-901.
pmid: 8159391
|
| [7] |
Miklos JR, Moore RD, Chinthakanan O. Laparoscopic and robotic-assisted vesicovaginal fistula repair: a systematic review of the literature. J Minim Invasive Gynecol 2015; 22:727-36.
pmid: 25764976
|
| [8] |
Schmitt A, Crochet P, Knight S, Tourette C, Loundou A, Agostini A. Single-port laparoscopy versus conventional laparoscopy in benign adnexal diseases: a systematic review and meta-analysis. J Minim Invasive Gynecol 2017; 24:1083-95.
doi: 10.1016/j.jmig.2017.07.001
pmid: 28705751
|
| [9] |
Lee KW, Choi SW, Park YH, Bae WJ, Choi YS, Ha US, et al. A randomized, prospective study of laparoendoscopic single-site plus one-port versus mini laparoscopic technique for live donor nephrectomy. World J Urol 2018; 36:585-93.
doi: 10.1007/s00345-018-2207-9
pmid: 29396785
|
| [10] |
Abdel-Karim AM, Moussa A, Elsalmy S. Laparoendoscopic single site surgery extravesical repair of vesicovaginal fistula: early experience. Urology 2011; 78:567-71.
doi: 10.1016/j.urology.2011.05.036
pmid: 21782221
|
| [11] |
Mahadevappa N, Gudage S, Senguttavan KV, Mallya A, Dharwadkar S. Laparoendoscopic single site surgery for extravesical repair of vesicovaginal fistula using conventional instruments: our initial experience. Urol Ann 2016; 8:305-11.
pmid: 27453652
|
| [12] |
Roslan M, Markuszewski M. Transvesical laparoendoscopic single-site approach for repair of urinary tract injuries after vaginal or pelvic surgery. Ginekol Pol 2014; 85:272-7.
pmid: 24834704
|
| [13] |
O’Conor VJ, Sokol JK. Vesicovaginal fistula from the standpoint of the urologist. J Urol 1951; 66:579-85.
pmid: 14881232
|
| [14] |
Rizvi SJ, Gupta R, Patel S, Trivedi A, Trivedi P, Modi P. Modified laparoscopic abdominal vesico-vaginal fistula repaird“Mini-O’Conor” vesicotomy. J Laparoendosc Adv Surg Tech A 2010; 20:13-5.
pmid: 20059325
|
| [15] |
Sharma AP, Mavuduru RM, Bora GS, Devana SK, Singh SK, Mandal AK. Robot-assisted vesico-vaginal fistula repair: a compilation. Urology 2018; 119:1-4.
pmid: 29894777
|
| [16] |
Ghosh B, Biswal DK, Bera MK, Pal DK. Laparoscopic vesicovaginal fistula repair with limited cystotomy: a rewarding treatment option. J Obstet Gynaecol India 2016; 66:370-6.
doi: 10.1007/s13224-015-0741-6
pmid: 27651632
|
| [17] |
Abdel-Karim AM, Mousa A, Hasouna M, Elsalmy S. Laparoscopic transperitoneal extravesical repair of vesicovaginal fistula. Int Urogynecol J 2011; 22:693-7.
doi: 10.1007/s00192-010-1334-7
pmid: 21107809
|
| [18] |
Miklos JR, Moore RD. Laparoscopic extravesical vesicovaginal fistula repair: our technique and 15-year experience. Int Urogynecol J 2015; 26:441-6.
pmid: 25027019
|
| [19] |
Javali TD, Katti A, Nagaraj HK. A simplified laparoscopic approach to repair vesicovaginal fistula: the M.S. Ramaiah technique. Urology 2015; 85:544-6.
pmid: 25586477
|
| [20] |
Ramphal SR. Laparoscopic approach to vesicovaginal fistulae. Best Pract Res Clin Obstet Gynaecol 2019; 54:49-60.
pmid: 30078652
|
| [21] |
Goyal NK, Dwivedi US, Vyas N, Rao MP, Trivedi S, Singh PB. A decade’s experience with vesicovaginal fistula in India. Int Urogynecol J Pelvic Floor Dysfunct 2007; 18:39-42.
doi: 10.1007/s00192-006-0068-z
pmid: 17006615
|
| [1] |
Lingfan Xu,Junyi Chen,Weipeng Liu,Chaozhao Liang,Hailiang Hu,Jiaoti Huang. Targeting androgen receptor-independent pathways in therapy-resistant prostate cancer[J]. Asian Journal of Urology, 2019, 6(1): 91-98. |
| [2] |
Zhang Yumeng,Zhang Kaile,Fu Qiang. Emergency treatment of male blunt urethral trauma in China: Outcome of different methods in comparison with other countries[J]. Asian Journal of Urology, 2018, 5(2): 78-87. |
| [3] |
Zou Qingsong,Fu Qiang. Tissue engineering for urinary tract reconstruction and repair: Progress and prospect in China[J]. Asian Journal of Urology, 2018, 5(2): 57-68. |
| [4] |
Ka Wing Wong, Terence Chun-ting Lai, Ada Tsui-lin Ng, Brian Sze-ho Ho, James Hok-leung Tsu, Chiu Fung Tsang, W. K. Ma, Ming Kwong Yiu. Anterior perineal hernia after anterior exenteration[J]. Asian Journal of Urology, 2017, 4(4): 253-255. |
| [5] |
Belinda Nghiem, Xiaotun Zhang, Hung-Ming Lam, Lawrence D. True, Ilsa Coleman, Celestia S. Higano, Peter S. Nelson, Colin C. Pritchard, Colm Morrissey. Mismatch repair enzyme expression in primary and castrate resistant prostate cancer[J]. Asian Journal of Urology, 2016, 3(4): 223-228. |
| [6] |
Victor C. Lin, Chung-hsien Chen, Allen W. Chiu, . Laparoscopic nephroureterectomy for upper tract urothelial carcinoma e Update[J]. Asian Journal of Urology, 2016, 3(3): 115-119. |
| [7] |
Zhixiang Wang, Bing Liu, Xiaofeng Gao, Yi Bao, Yang Wang, Huamao Ye, Yinghao Sun, Linhui Wang. Laparoscopic ureterolysis with simultaneous ureteroscopy and percutaneous nephroscopy for treating complex ureteral obstruction after failed endoscopic intervention: A technical report[J]. Asian Journal of Urology, 2015, 2(4): 238-243. |
| [8] |
Sammy E. Elsamra, Nikhil Gupta, Haris Ahmed, David Leavitt, Jessica Kreshover, Louis Kavoussi, Lee Richstone. Robotic assisted laparoscopic simple suprapubic prostatectomy—The Smith Institute for urology experience with an evolving technique[J]. Asian Journal of Urology, 2014, 1(1): 52-56. |
|
|
|
|