|
|
|
| Lingual mucosal graft urethroplasty 12 years later: Systematic review and meta-analysis |
Alberto Abratea,Andrea Gregorib,Alchiede Simonatoa,*( ) )
|
aDepartment of Surgical, Oncological and Oral Sciences, Section of Urology, University of Palermo, Palermo, Italy
bDepartment of Urology, ASST Rhodense, G. Salvini Hospital, Garbagnate Milanese, Milan, Italy |
|
|
|
|
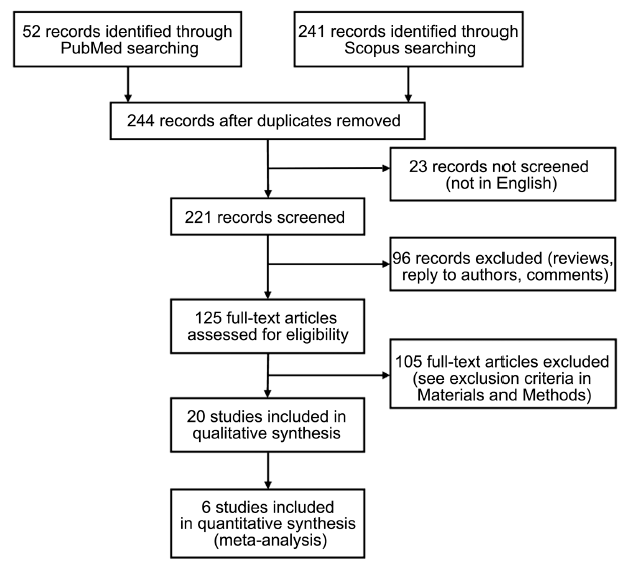
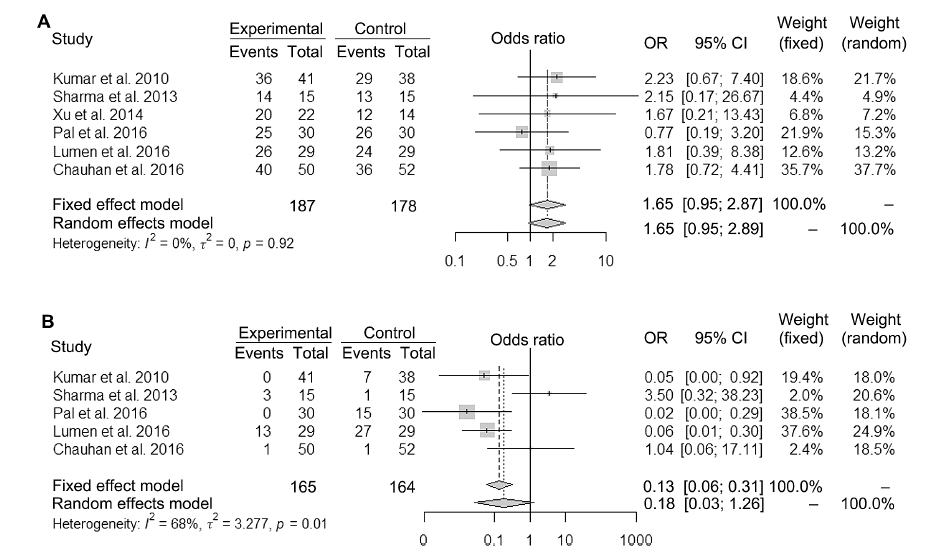
Abstract Objective: To evaluate the functional results and complications of the lingual mucosal graft (LMG) urethroplasty and to sum up the current state of the art of this surgical technique. Methods: A systematic search of PubMed and Scopus electronic databases was performed, according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. Studies involving male patients treated with LMG urethroplasty for urethral stricture were included. Complete protocol is available at http://www.crd.york.ac.uk/PROSPERO/display_record.php?ID=CRD42017080121. A meta-analysis comparing functional and long-term oral complication outcomes of LMG and buccal mucosal graft (BMG) was performed, calculating the odds ratio (OR) and 95% confidence interval (CI). Results: Twenty original articles were included in the qualitative analysis. Strictures of 1.5-16.5 cm have been treated with LMG urethroplasty, due to the improvement of harvesting technique and very low rate of long-term oral complications. Very good functional results have been reported by different authors for LMG urethroplasty, with lower rate of oral complications than BMG. The meta-analysis included six comparative studies involving 187 and 178 patients treated with LMG and BMG urethroplasty, respectively. An OR of 1.65 (95% CI [0.95-2.87], I 2 = 0%) and 0.18 (95% CI [0.03-1.26], I 2 = 68%) were found for LMG vs. BMG urethroplasty, in terms of success and oral complication rate, respectively. Conclusion: LMG urethroplasty can be reasonably considered a first choice technique for urethral stricture with very good results. Oral complications are temporary and minimally disabling, basically less than those for BMG, and depend mainly on the graft extent.
|
|
Received: 29 June 2018
Available online: 09 January 2019
|
|
Corresponding Authors:
Alchiede Simonato
E-mail: alchiede@gmail.com
|
|
|
|
|
Flow of information through the different phases of the systematic review.
|

| Author [Ref.] | Type of study | Patients, n (LMG) | Type of graft | Follow-up, month (range) | LE | | Sharma et al., 2013 [17] | Prospective randomized controlled study | 30 (15) | LMG vs. BMG | 15.2 (NA) | 2 | | Chauhan et al., 2016 [20] | Prospective randomized controlled study | 102 (50) | LMG vs. BMG | 25 (12-52) | 2 | | Lumen et al., 2016 [18] | Prospective non-randomised controlled cohort study | 58 (29) | LMG vs. BMG | 30 (NA) | 3 | | Pal et al., 2016 [21] | Prospective non-randomised controlled cohort study | 60 (30) | LMG vs. BMG | 14.1 (7-19) | 3 | | Sharma et al., 2016 [26] | Prospective non-randomised study | 12 (12) | LMG | 11.6 (6-14) | 3 | | Simonato et al., 2006 [8] | Retrospective case series | 8 (8) | LMG | 18 (NA) | 4 | | Kumar et al., 2007 [22] | Retrospective case series | 30 (30) | LMG | 3.8 (NA) | 4 | | Simonato et al., 2008 [11] | Retrospective case series | 29 (27) | LMG or LMG + BMG | 17.7 (6-71) | 4 | | Singh et al., 2008 [12] | Retrospective comparative study | 55 (55) | LMG | 13-22 (NA) | 4 | | Barbagli et al., 2008 [16] | Retrospective case series | 10 (10) | LMG | 5 (3-12) | 4 | | Kumar et al., 2008 [29] | Retrospective case series | 25 (25) | LMG | 4.2 (2.5-7.4) | 4 | | Das et al., 2009 [13] | Retrospective case series | 30 (30) | LMG | 9 (4-12) | 4 | | Xu et al., 2010 [25] | Retrospective case series | 92 (76) | LMG or LMG + foreskin flap or LMG + BMG | 17.2 (3-33) | 4 | | Kumar et al., 2010 [15] | Retrospective comparative study | 79 (41) | LMG vs. BMG | 17.5 (12-26) | 4 | | Xu et al., 2011 [24] | Retrospective case series | 110 (110) | LMG | 22 (6-41) | 4 | | Xu et al., 2014 [14] | Retrospective case series | 36 (22) | LMG vs. BMG vs. LMG + BMG | 38.7 (12-110) | 4 | | Abdelhameed et al., 2015 [27] | Retrospective case series | 23 (23) | LMG | 66 (60-72) | 4 | | Zhang et al., 2016 [28] | Retrospective case series | 101 (101) | LMG | 23 (13-37) | 4 | | Xu et al., 2017 [23] | Retrospective case series | 81 (69) | LMG or LMG + BMG | 41 (15-86) | 4 | | Fu et al., 2017 [19] | Retrospective comparative study | 293 (94) | LMG vs. skin flap | 12 (NA) | 4 |
|
|
Quality assessment of the studies included in the systematic review, ordered by LE.
|
| Author [Ref.] | Stricture length, mean (range), cm | Follow-up method | Definition of failure | Success rate, % | Urethral complications, n (%) | | Simonato et al., 2006 [8] | 3.1 (1.5-4.5) | Uroflowmetry 3 and 12 mo
Urethrography 2 weeks, 3 and 12 mo
Urethroscopy 3 and 12 mo | Qmax <15 mL/s
Need for any instrumentation | 87.5 | Stricture recurrence 6 (20.7)
Contrast extravasation, 2 (6.9) | | Simonato et al., 2008 [11] | 3.6 (1.5-9.8) | Uroflowmetry 3 and 12 mo
Urethrography 2 weeks, 3 and 12 mo
Urethroscopy 3 and 12 mo | Inability to void
Post void residual
Need for any instrumentation | 81.5 | NA | | Singh et al., 2008 [12] | 10.2 (3.7-16.5)
9.8 (3.5-12.9) | Uroflowmetry 3, 6 and 12 mo
Urethrography 3, 6 and 12 mo | Need for any instrumentation | 76.6-80 | Meatal narrowing, 8 (14.5)
Stricture recurrence, 7 (12.7)
Contrast extravasation, 3 (5.5)
Wound infection, 3 (5.5)
Penis curvature, 1 (1.8) | | Barbagli et al., 2008 [16] | NA | Uroflowmetry 4, 8 and 12 mo
Urethrography if needed
Urethroscopy if needed
Urethral ultrasound if needed | Need for any instrumentation | 90 | Contrast extravasation, 1 (10)
Stricture recurrence, 1 (10) | | Das et al., 2009 [13] | 10.2 (3.7-16.5) | Uroflowmetry 3 and 6 mo
Urethrography 3 weeks, 3 and 6 mo | Qmax <15 mL/s
Need for any instrumentation | 83.3 | Contrast extravasation, 5 (16.7)
Wound infection, 2 (6.7)
Haematoma, 2 (6.7)
Stricture recurrence, 1 (3.3)
Meatal stenosis, 4 (13.3)
Penis curvature 1 (3.3) | | Xu et al., 2010 [25] | 6.5 (2.5-18.0) | Uroflowmetry 3, 6, 12, 18, 24 and 36 mo
Urethrography if needed
Urethroscopy if needed | Need for any instrumentation | 91.3 | Contrast extravasation, 4 (4.3)
Stricture recurrence, 4 (4.3) | | Kumar et al., 2010 [15] | 8.8 (4.0-16.5) | Uroflowmetry 3, 6 and 12 mo
Urethrography 3, 6 and 12 mo | Qmax <15 mL/s
Need for any instrumentation | 87.8 | Contrast extravasation, 6 (14.6)
Stricture recurrence, 5 (12.2)
Meatal stenosis, 5 (12.2)
Wound infection, 3 (7.3) | | Sharma et al., 2013 [17] | 7.7 (3.2-9.6) | Uroflowmetry 3 weeks, 3, 6, 12 mo
Urethrography 3 mo
Urethroscopy 6 mo | Qmax <10 mL/s
Residual stricture
Need for any instrumentation | 93.3 | NA | | Xu et al., 2014 [14] | 12.5 (6.0-18.0) | Urethrography 4 weeks
Uroflowmetry 3, 6, 12, 24, and 36 mo | Qmax <12 mL/s
Obstructive symptoms
Need for any instrumentation | 90.9 | Meatal stenosis, 2/22 (9.1) LMG
Fistula, 1/9 (11.1) LMG + BMG | | Abdelhameed et al., 2015 [27] | 4.6 (3.0-11.5) | Uroflowmetry 3, 6, 12, 24, 36, 48 and 60 mo
Urethrography 3 and 6 mo | Obstructive symptoms
Residual stricture
Need for any instrumentation | 86.9 | Contrast extravasation, 1 (4.3)
Wound infection, 4 (17.4)
Postvoid dribbling, 3 (13.0) | | Pal et al., 2016 [21] | 9.6 (3.5-15.5) | Uroflowmetry 3 and 6 mo
Urethrography if needed | Qmax <15 mL/s
Significant postvoid residual volume
Need for major instrumentation | 83.3 | Contrast extravasation, 5/30 (16.7)
Stricture recurrence, 2/30 (6.7)
Meatal stenosis, 4/30 (13.3)
Haematoma, 1/30 (3.3) | | Sharma et al., 2016 [26] | 4.7 (3.0-8.5) | Urine analysis 1, 3, 6 and 12 mo
Uroflowmetry 1, 3, 6 and 12 mo
Postvoid residual assessment 1, 3, 6 and 12 mo
Urethrocystoscopy 3 mo | Need for any instrumentation | 91.6 | Stricture recurrence, 1 (8.3) | | Lumen et al., 2016 [18] | 5.0 (1.0-16.0) | Uroflowmetry
Urethrography if needed
Urethroscopy if needed | Stricture recurrence or fistula
Need for any instrumentation | 89.7 | Stricture recurrence, 2/29 (6.9)
Fistula, 1/29 (3.4) | | Chauhan et al., 2016 [20] | 6.7 (3.8-12.2) | Uroflowmetry 1, 3 and 6 mo
Urethrography if needed
Urethroscopy if needed | Obstructive symptoms
Need for any instrumentation | 80 | NA | | Zhang et al., 2016 [28] | 7.0 (2.0-16.0) | Uroflowmetry 4 weeks, 3, 6, 12, 24 and 36 mo
Urethrography 4 weeks, 3, 6, 12, 24 and 36 mo | Stricture recurrence
Fistula | 81.2 | Stricture recurrence, 17 (16.8)
Fistula, 2 (2.0) | | Xu et al., 2017 [23] | 12.1 (8.0-20.0) | Urethrography 4 weeks
Uroflowmetry 3, 6, 12, 18 and 24 mo
Urethrography if needed
Urethroscopy if needed | Qmax <12 mL/s
Obstructive symptoms
Need for any instrumentation | 82.7 | Stricture recurrence, 10 (12.3)
Fistula, 4 (4.9) | | Fu et al., 2017 [19] | 4.9 (1.5-12.0) | Uroflowmetry 3 weeks, 3 and 12 mo | Qmax <12 mL/s
Fistula or diverticulum
Obstructive symptoms
Need for any instrumentation | 85.1 | NA |
|
|
Functional results and urethral complications of LMG urethroplasty.
|
| Author [Ref.] | Graft length, mean (range), cm | Immediate complications, n (%) | Long-term complications, n (%) | | Simonato et al., 2006 [8] | 3.3 (3.0-7.0) | Oral discomfort, all (100) | None | | Kumar et al., 2007 [22] | 8.5 (4.2-16.2) | Pain, 28 (93.3)
Slurring speech, 6 (20) | None | | Kumar et al., 2008 [29] | 6.5 (3.5-16.4) | Pain, 23 (92)
Slurring speech, 6 (24) | None | | Simonato et al., 2008 [11] | NA | Oral discomfort, all (100)
Slurring speech, all (100)
Difficulty in mouth opening, 2 (100) LMG + BMG
Reduced slivatory flow, 1 (50) LMG + BMG
Neurosensory deficit, 2 (100) LMG + BMG | None | | Das et al., 2009 [13] | 10.7 (3.9-17.0) | Pain, all (100)
Slurring speech, all (100) | None | | Xu et al., 2010 [25] | NA (4.0-14.0) | Oral discomfort, all (100)
Difficulty in moving the tongue, all (100) | Numbness, 10 (13.2) | | Kumar et al., 2010 [15] | 9.2 (4.5-17.0) | Pain, 38 (92.7)
Slurring speech, 9 (21.9)
Numbness, 2 (4.9)
Salivatory disturbance, 1 (2.4)
Delayed feeding, 1 (2.4) | None | | Xu et al., 2011 [24] | 5.2 (3.0-7.0)
11.5 (7.5-14.5) | Pain, 105 (95.4)
Delayed feeding, 8 (17.6) bilateral graft
Difficulty in moving the tongue, 14 (48.3) bilateral graft
Numbness, 35 (31.8)
Parageusia, 12 (10.9)
Slurring speech, 38 (34.5) | Numbness, 7 (6.4)
Parageusia, 3 (2.7)
Slurring speech, 3 (2.7) | | Sharma et al., 2013 [17] | NA | Bleeding, 1 (6.7)
Pain, all (100)
Swelling of the tongue, 2 (13.3)
Difficulty in opening the mouth, 2 (13.3)
Difficulty in tongue protrusion, all (100)
Swallowing, all (100)
Difficulty in chewing, all (100)
Speech difficulty, all (100)
Numbness, 6 (40) | Difficulty in tongue protrusion, 2 (13.3)
Speech difficulty, 3 (20) | | Xu et al., 2014 [14] | NA (7.0-15.0) | Pain, all (100)
Difficulty in moving the tongue, all (100) | None | | Abdelhameed et al., 2015 [27] | 5.6 (4.0-12.0) | Oral discomfort, all (100)
Difficulty in moving the tongue, all (100)
Speech difficulty, all (100)
Numbness, 9 (39.1) | None | | Pal et al., 2016 [21] | 10.1 (4.8-16.2) | Pain, 27 (90)
Difficulty in moving the tongue, 11 (36.7)
Slurring speech, 11 (36.7) | None | | Chauhan et al., 2016 [20] | NA | Pain, 20 (40)
Bleeding, 8 (16)
Difficulty in chewing, 24 (48)
Swelling of the tongue, 13 (26)
Difficulty in articulation, 22 (44)
Difficulty in opening the mouth, 19 (38)
Dry mouth, 7 (14)
Sensitivity disorders, 23 (46) | Difficulty in articulation, 1 (2) | | Lumen et al., 2016 [18] | 5.0 (1.0-20.0) | Pain, 17 (58.6)
Difficulty in eating, 18 (62.1)
Sensitivity disorders, 21 (72.4)
Speech difficulty, 27 (93.1)
Dysgeusia, 14 (48.3) | Difficulty in eating solids, 1 (3.4)
Oral tightness, 1 (3.4)
Sensitivity disorders, 9 (31)
Salivary changes, 2 (6.9)
Speech difficulty, 4 (13.8)
Dysgeusia, 1 (3.4) | | Zhang et al., 2016 [28] | 7.2 (2.5-16.0) | Pain, all (100)
Numbness, 25 (24.7) | Numbness, 5 (5.5)
Slurring speech, 5 (5.5)
Swallowing dysfunction, 5 (5.5)
Parageusia, 3 (3.3) | | Xu et al., 2017 [23] | NA (9.0-17.0) | Pain, all (100)
Difficulty in moving the tongue, all (100) | Numbness, 4 (4.9)
Slurring speech, 2 (2.5)
Difficulty in moving the tongue, 5 (6.2) |
|
|
Donor site complications after lingual mucosa harvesting: Post-operative and 1 year after surgery (or at the end of the follow-up period).
|

|
|
Fundamental steps of the surgical technique for LMG urethroplasty. (A) Patient is placed in lithotomy position under general anesthesia with naso-tracheal intubation. Urethra is probed with a catheter to detect the stricture. (B) The stenotic urethra is completely mobilized from the corpora cavernosa after a complete degloving of the penis (in case of long penile urethroplasty) or a perineoscrotal incision (in case of bulbar urethroplasty). The strictured tract is fully opened by a ventral midline incision and carefully measured. The urethral plate is longitudinally incised on the dorsal midline down to the corpora and the wings of the urethral plate are laterally mobilized. (C) LMG harvesting can be started during the latter part of the urethral mobilization or at the same time by two teams. A silicone bite block prop—mouth opener—is placed. (D) Direct traction is applied with two Babcock clamps to expose the ventrolateral surface of the tongue. A surgical pen is used to mark the required graft after identification of the opening of the Warton duct. (E) The graft edges are incised with a scalpel and a full-thickness mucosal graft is harvested using sharp scissors. Although a graft of 7-8 cm can be easily harvested from one half of the tongue, it should be at least 2 cm longer than the measured stricture length and 15-25 mm wide. Thus for long strictures the procedure can be repeated on the contralateral side. After the lingual mucosa is harvested, the wound is closed with interrupted polyglactin 4-0 sutures, without excessive tension. (F) Lingual mucosa is then prepared completely removing the underlying fibrovascular tissue. (G) The LMG is sutured and quilted on the bed of the dorsal urethral incision with tension free, interrupted, absorbable and at least 4-0 sutures, and an augmentation of the urethral plate is obtained. (H) The urethra is closed and tubularized over an indwelling 14Ch silicone catheter. A dartos fascial flap is obtained to cover the urethral suture. (I) The glans and penile skin are closed with interrupted 3-0 absorbable sutures. A Foley 14Ch silicone catheter should be left in place for at least 3 weeks. LMG, lingual mucosal graft.
|
|
|
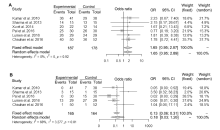
Forest plot of OR (95% CI) for success rate (A) and long-term oral complications (B) of LMG (Experimental) vs. BMG (Control) urethroplasty. The center of each square represents the OR, the area of the square is the number of samples and thus the weight used in the meta-analysis and the horizontal line indicates the 95% CI. LMG, lingual mucosal graft; BMG, buccal mucosal graft; OR, odds ratio; CI, confidence interval.
|
|
|
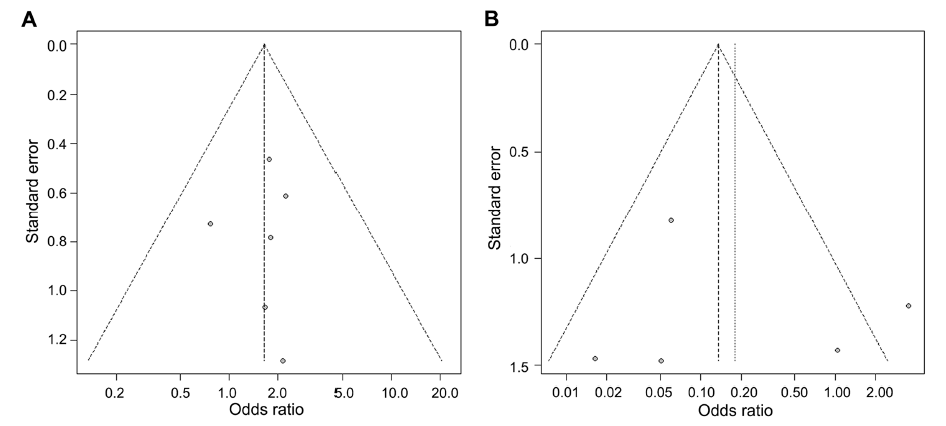
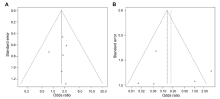
Funnel plots for publication bias. (A) Six studies analyzing success rate of LMG vs. BMG urethroplasty; (B) Five studies analyzing long-term oral complication rate of LMG vs. BMG urethroplasty. LMG, lingual mucosal graft; BMG, buccal mucosal graft.
|
| [1] |
Jordan GH . Scrotal and perineal flaps for anterior urethral reconstruction. Urol Clin North Am 2002; 29:411-6.
|
| [2] |
Kinkead TM, Borzi PA, Duffy PG, Ransley PG . Long-term followup of bladder mucosa graft for male urethral reconstruction. J Urol 1994; 151:1056-8.
|
| [3] |
Xu YM, Qiao Y, Sa YL, Zhang J, Fu Q, Song LJ . Urethral reconstruction using colonic mucosa graft for complex strictures. J Urol 2009; 182:1040-3.
|
| [4] |
Manoj B, Sanjeev N, Pandurang PN, Jaideep M, Ravi M . Postauricular skin as an alternative to oral mucosa for anterior onlay graft urethroplasty: a preliminary experience in patients with oral mucosa changes. Urology 2009; 74:345-8.
|
| [5] |
Simonato A, Gregori A . Lingual mucosal grafts for anterior urethroplasty: a review. BJU Int 2010; 105:132-3.
|
| [6] |
Bhargava S, Chapple CR . Buccal mucosal urethroplasty: is it the new gold standard? BJU Int 2004; 93:1191-3.
|
| [7] |
Wood DN, Allen SE, Andrich DE, Greenwell TJ, Mundy AR . The morbidity of buccal mucosal graft harvest for urethroplasty and the effect of nonclosure of the graft harvest site on postoperative pain. J Urol 2004; 172:580-3.
|
| [8] |
Simonato A, Gregori A, Lissiani A, Galli S, Ottaviani F, Rossi R , et al. The tongue as an alternative donor site for graft urethroplasty: a pilot study. J Urol 2006; 175:589-92.
|
| [9] |
Moher D, Liberati A, Tetzlaff J, Altman DG . Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med 2009; 6:e1000097.
|
| [10] |
OCEBM Levels of Evidence Working Group The Oxford 2011 levels of evidence Oxford Centre for Evidence-Based Medicine. [accessed 25 February 2018]. .
|
| [11] |
Simonato A, Gregori A, Ambruosi C, Venzano F, Varca V, Romagnoli A , et al. Lingual mucosal graft urethroplasty for anterior urethral reconstruction. Eur Urol 2008; 54:79-85.
|
| [12] |
Singh PB, Das SK, Kumar A, Sharma GK, Pandey AK, Swain S , et al. Dorsal onlay lingual mucosal graft urethroplasty: comparison of two techniques. Int J Urol 2008; 15:1002-5.
|
| [13] |
Das SK, Kumar A, Sharma GK, Pandey AK, Bansal H, Trivedi S , et al. Lingual mucosal graft urethroplasty for anterior urethral strictures. Urology 2009; 73:105-8.
|
| [14] |
Xu YM, Feng C, Sa YL, Fu Q, Zhang J, Xie H . Outcome of 1-stage urethroplasty using oral mucosal grafts for the treatment of urethral strictures associated with genital lichen sclerosus. Urology 2014; 83:232-6.
|
| [15] |
Kumar A, Das SK, Trivedi S, Dwivedi US, Singh PB . Substitution urethroplasty for anterior urethral strictures: buccal versus lingual mucosal graft. Urol Int 2010; 84:78-83.
|
| [16] |
Barbagli G, De Angelis M, Romano G, Ciabatti PG, Lazzeri M . The use of lingual mucosal graft in adult anterior urethroplasty: surgical steps and short-term outcome. Eur Urol 2008; 54:671-6.
|
| [17] |
Sharma AK, Chandrashekar R, Keshavamurthy R, Nelvigi GG, Kamath AJ, Sharma S , et al. Lingual versus buccal mucosa graft urethroplasty for anterior urethral stricture: a prospective comparative analysis. Int J Urol 2013; 20:1199-203.
|
| [18] |
Lumen N, Vierstraete-Verlinde S, Oosterlinck W, Hoebeke P, Palminteri E, Goes C , et al. Buccal versus lingual mucosa graft in anterior urethroplasty: a prospective comparison of surgical outcome and donor site morbidity. J Urol 2016; 195:112-7.
|
| [19] |
Fu Q, Zhang Y, Zhang J, Xie H, Sa YL, Jin S . Substitution urethroplasty for anterior urethral stricture repair: comparison between lingual mucosa graft and pedicled skin flap. Scand J Urol 2017; 51:479-83.
|
| [20] |
Chauhan S, Yadav SS, Tomar V . Outcome of buccal mucosa and lingual mucosa graft urethroplasty in the management of urethral strictures: a comparative study. Urol Ann 2016; 8:36-41.
|
| [21] |
Pal DK, Gupta DK, Ghosh B, Bera MK . A comparative study of lingual mucosal graft urethroplasty with buccal mucosal graft urethroplasty in urethral stricture disease: an institutional experience. Urol Ann 2016; 8:157-62.
|
| [22] |
Kumar A, Goyal NK, Das SK, Trivedi S, Dwivedi US, Singh PB . Oral complications after lingual mucosal graft harvest for urethroplasty. ANZ J Surg 2007; 77:970-3.
|
| [23] |
Xu YM, Li C, Xie H, Sa YL, Fu Q, Wu DL , et al. Intermediateterm outcomes and complications of long segment urethroplasty with lingual mucosa grafts. J Urol 2017; 198:401-6.
|
| [24] |
Xu YM, Xu QK, Fu Q, Sa YL, Zhang J, Song LJ , et al. Oral complications after lingual mucosal graft harvesting for urethroplasty in 110 cases. BJU Int 2011; 108:140-5.
|
| [25] |
Xu YM, Fu Q, Sa YL, Zhang J, Jin CR, Si JM , et al. Treatment of urethral strictures using lingual mucosas urethroplasty: experience of 92 cases. Chin Med J (Engl) 2010; 123:458-62.
|
| [26] |
Sharma U, Yadav SS, Tomar V, Garg A . Single stage circumferential lingual mucosal graft urethroplasty in near obliterative bulbar urethra stricture: a novel technique. Urol Ann 2016; 8:146-50.
|
| [27] |
Abdelhameed H, Elgamal S, Farha MA, El-Abd A, Tawfik A, Soliman M . The long-term results of lingual mucosal grafts for repairing long anterior urethral strictures. Arab J Urol 2015; 13:128-33.
|
| [28] |
Zhang K, Zhou S, Zhang Y, Xu Y, Jin S, Sa Y , et al. Anterior urethra reconstruction with lateral lingual mucosa harvesting technique. Urology 2016; 90:208-12.
|
| [29] |
Kumar A, Das SK, Sharma GK, Pandey AK, Trivedi S, Dwivedi US , et al. Lingual mucosal graft substitution urethroplasty for anterior urethral strictures: our technique of graft harvesting. World J Urol 2008; 26:275-80.
|
| [30] |
Chapple C, Andrich D, Atala A, Barbagli G, Cavalcanti A, Kulkarni S , et al. SIU/ICUD Consultation on Urethral Strictures: the management of anterior urethral stricture disease using substitution urethroplasty. Urology 2014; 83(Suppl. 3):S31-47.
|
| [31] |
Mangera A, Osman N, Chapple C . Evaluation and management of anterior urethral stricture disease. F1000Res 2016; 9:5.
|
| [32] |
Djordjevic ML . Graft surgery in extensive urethral stricture disease. Curr Urol Rep 2014; 15:424.
|
| [33] |
Maarouf AM, Elsayed ER, Ragab A, Salem E, Sakr AM, Omran M , et al. Buccal versus lingual mucosal graft urethroplasty for complex hypospadias repair. J Pediatr Urol 2013; 9:754-8.
|
| [34] |
Elsayed E, Dawod T, Abdalla M, Teleb M, Teelab A, Omran M , et al. One-stage lingual augmented urethroplasty in repair of distal penile hypospadias. Afr J Urol 2015; 21:6-9.
|
| [35] |
Hongyong J, Shuzhu C, Min W, Weijing Y, Yidong L . Comparison of lingual mucosa and buccal mucosa grafts used in inlay urethroplasty in failed hypospadias of pre-pubertal boys in a Chinese group. PLoS One 2017; 12:e0182803. .
|
| [36] |
Sharma GK, Pandey A, Bansal H, Swain S, Das SK, Trivedi S , et al. Dorsal onlay lingual mucosal graft urethroplasty for urethral strictures in women. BJU Int 2010; 105:1309-12.
|
| [37] |
Kumar N, Bhardwaj A, Negi PC, Jhingta PK, Sharma D, Bhardwaj VK . Association of chronic periodontitis with metabolic syndrome: a cross-sectional study. J Indian Soc Periodontol 2016; 20:324-9.
|
| [1] |
Guido Barbagli,Axel Heidenreich,Vahudin Zugor,Leonidas Karapanos,Massimo Lazzeri. Urothelial or oral mucosa cells for tissue-engineered urethroplasty: A critical revision of the clinical outcome[J]. Asian Journal of Urology, 2020, 7(1): 18-23. |
| [2] |
Tapan K. Mandal,Shashanka Dhanuka,Sunirmal Choudhury,Bibhas C. Mukhopadhyay,Ankit Kayal,Tapas K. Majhi,Maharaj Mondal. Tissue engineered indigenous pericardial patch urethroplasty: A promising solution to a nagging problem[J]. Asian Journal of Urology, 2020, 7(1): 56-60. |
| [3] |
Shi Qiu,Siwei Bi,Tianhai Lin,Zhuheng Wu,Qi’an Jiang,Jiwen Geng,Liangren Liu,Yige Bao,Xiang Tu,Mingjing He,Lu Yang,Qiang Wei. Comparative assessment of efficacy and safety of different treatment for de novo overactive bladder children: A systematic review and network meta-analysis[J]. Asian Journal of Urology, 2019, 6(4): 330-338. |
| [4] |
Reem Aldamanhori,Richard Inman. The treatment of complex female urethral pathology[J]. Asian Journal of Urology, 2018, 5(3): 160-163. |
| [5] |
Emilio Ríos,Luís Martínez-Pi?eiro. Treatment of posterior urethral distractions defects following pelvic fracture[J]. Asian Journal of Urology, 2018, 5(3): 164-171. |
| [6] |
Simsek Abdulmuttalip,Aldamanhori Reem,R.Chapple Christopher,MacNeil Sheila. Overcoming scarring in the urethra: Challenges for tissue engineering[J]. Asian Journal of Urology, 2018, 5(2): 69-77. |
| [7] |
Cheng Li,Li Sen,Wang Zicheng,Huang Bingwei,Lin Jian. A brief review on anterior urethral strictures[J]. Asian Journal of Urology, 2018, 5(2): 88-93. |
| [8] |
Guido Barbagli, Sofia Balò, Francesco Montorsi, Salvatore Sansalone, Massimo Lazzeri. History and evolution of the use of oral mucosa for urethral reconstruction[J]. Asian Journal of Urology, 2017, 4(2): 96-101. |
| [9] |
Ka Wing Wong, Brian Sze Ho Ho, Chi Ho Ip, Ming Kwong Yiu. Isolated penile urethral injury: A rare case following male coital trauma[J]. Asian Journal of Urology, 2015, 2(3): 175-178. |
| [10] |
Christopher J. Hillary, Nadir I. Osman, Christopher R. Chapple. Current trends in urethral stricture management[J]. Asian Journal of Urology, 2014, 1(1): 44-51. |
|
|
|
|