|
|
|
| Compliance in patients with dietary hyperoxaluria: A cohort study and systematic review |
Derek B. Hennesseya,b,*( ),Ned Kinnearb,Gilbert Ricea,David Currya,Siobhan Woolseya,Brian Duggana,c ),Ned Kinnearb,Gilbert Ricea,David Currya,Siobhan Woolseya,Brian Duggana,c
|
a.Department of Urology, Belfast City Hospital, Belfast, United Kingdom;
b.Department of Urology, Austin Hospital, Melbourne, Australia;
c.Department of Urology, Ulster Hospital, Belfast, United Kingdom |
|
|
|
|
Abstract Objective Hyperoxaluria leads to calcium oxalate crystal formation and subsequent urolithiasis. This study aims to analyse the effect of treatment compliance in hyperoxaluria, firstly by analysis of patients with non-primary hyperoxaluria and secondly via systematic review in patients with any hyperoxaluria.Methods In a retrospective cohort study, adults with non-primary hyperoxaluria managed with dietary counselling in 2013 were enrolled. Twenty-four-hour (24 h) urine collections initially and at 6 months were obtained. Compliance was assessed by self-reported dietary compliance and 24 h urinary volume >2 L. Patients were followed for 24 months. Primary outcomes were urinary oxalate and calcium 24 h load at 6 months, and urolithiasis-related procedural rates at 24 months. A Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)-compatible systematic review of compliance among hyperoxaluric patients was performed.Results In the cohort study, of 19 eligible patients (4 female) with median age 52 years, 10 (53%) were considered compliant. Compared with the non-compliant group, these patients had significantly increased subsequent 24 h urinary volume (2250 mL vs. 1600 mL; p = 0.008) and lower procedural rates (10% vs. 56%; p = 0.033). Subsequent 24 h urinary oxalate load was non-significantly lower in compliant patients. Systematic review regarding compliance in hyperoxaluric patients revealed five studies. Only one utilised dietary counselling or analysed compliant vs. non-compliant patients, finding no difference. None examined the effect of compliance on procedural rates.Conclusion Hyperoxaluria is an important cause of recurrent urolithiasis. Increasing fluid intake and reducing dietary oxalate reduce the risk of operative intervention and remain fundamental to the treatment of hyperoxaluria.
|
|
Received: 02 April 2017
Available online: 29 March 2018
|
|
Corresponding Authors:
Derek B. Hennessey
E-mail: derek.hennessey@gmail.com
|
|
|

| Characteristics | Values | | Total number | 19 | | Age (year)a | 52 (45-60) | | Sex | | Male | 15 (79%) | | Female | 4 (21%) | | Lithogenic medical conditions (n = 14) | | Diabetes mellitus | 1 (7.25%) | | Hypercalcaemia | 1 (7.25%) | | Hyperuricaemia | 2 (12.751%) | | Recurrent UTI | 2 (12.75%) | | Malabsorptive disorders | 4 (28.5%) | | Renal anatomical abnormalities | 4 (28.5%) | | Non-operative treatment compliance | | Self-reported reduced dietary oxalate | 16 (84%) | | Increased fluid intake | 12 (63%) | | Both dietary and fluid measures | 10 (53%) | | Thiazide diuretics (n = 4) | 4 (100%) | | Stone analysis (n = 15) | | Calcium oxalate | 4 (26%) | | Calcium oxalate/apatate | 7 (47%) | | Calcium oxalate/apatate/magnesium phosphate | 3 (20%) | | Calcium oxalate/magnesium phosphate | 1 (7%) |
|
|
Patient characteristics.
|
| Parameter | Values | | Indications for 24 h collection, n (%) | | | Paediatric onset | 4 (21) | | Family history | 2 (11) | | Recurring stone disease | 7 (36) | | Bilateral stones | 2 (11) | | Medical disorder | 4 (21) | | 24 h urine collection, median (IQR) | | | Volume (mL) | 1550 (1400-2000) | | Oxalate (mmol/L) | 0.54 (0.49-0.68) | | Calcium (mmol/L) | 5.69 (2.64-9.76) | | Citrate (mmol/L) | 3.47 (1.6 0-5.15) | | Phosphate (mmol/L) | 30.13 (20.25-43.65) | | Urate (mmol/L) | 3.26 (2.34-4.57) | | Creatinine (mmol/L) | 13.45 (7.45-16.10) | | pH | 6.50 (5.675-6.80) | | Sodium (mmol/L) | 138.00 (78.00-208.50) | | Potassium (mmol/L) | 85.00 (53.75-109.50) | | Chloride (mmol/L) | 130.00 (84.00-193.50) | | Protein (mmol/L) | 0.08 (0.04-0.14) |
|
|
First 24 h collection indications and findings.
|
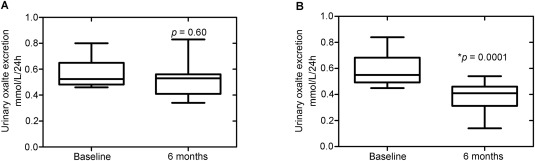
| Compliant | Non-compliant | p-Value | | Initial Collection | | Volume (mL) | 1643 (1250-1938) | 1400 (1400-1800) | 1 | | Oxalate (mmol/L) | 0.55 (0.51-0.63) | 0.53 (0.49-0.68) | 0.97 | | Citrate (mmol/L) | 3.17 (2.69-4.93) | 4.07 (1.38-6.08) | 1 | | Calcium (mmol/L) | 5.09 (2.46-6.38) | 7.28 (3.44-9.76) | 0.45 | | Subsequent collection | | Volume (mL) | 2250 (2000-2400) | 1600 (1200-1700) | 0.008 | | Oxalate (mmol/L) | 0.41 (0.34-0.46) | 0.53 (0.43-0.55) | 0.066 | | Citrate (mmol/L) | 2.92 (2.13-3.61) | 3.95 (2.22-5.17) | 0.55 | | Calcium (mmol/L) | 4.21 (2.91-6.81) | 7.14 (4.96-7.77) | 0.35 |
|
|
Comparison of initial and subsequent 24 h urine collection results between compliant and non-compliant groups, median (IQR).
|

|
|
Impact of compliance on 24 h urinary oxalate excretion. (A) Non complaint (n = 9); (B) Complaint patients (n = 10).
|

|
|
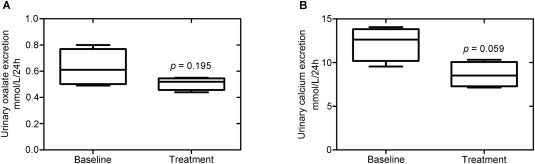
Effect at 6 months of thiazide diuretics on 24 h urinary oxalate and calcium excretion. (A) Urinary oxalate 24 h excretion; (B) Urinary calcium 24 h excretion.
|
|
|
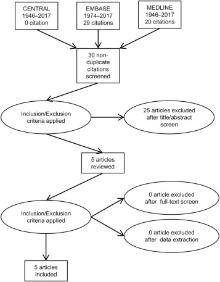
PRISMA flow diagram of citations reviewed in the course of systematic review of compliance to intervention in patients with hyperoxaluria. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
|
| Year | Author | Nation | Population | Methods | N | Outcomes | | 2013 | Schwen et al. [19] | USA | Adults with idiopathic hyperoxaluria, renal stones, at least two 24 h urine collections >30 days apart and non-operative management | Retrospective cohort study with contemporary controls. Oxalate-avoidant dietary counselling was given. Compliance was measured by self-reporting, improvement in urine volume and ability to keep follow-up appointments. | 149 | 132/149 (89%) compliant. Overall, mean UrOx was significantly reduced (p < 0.001), however no difference between compliant and non-compliant UrOx (p = 0.84). | | 2011 | Hoppe et al. [20] | Germany | Children and adults with primary hyperoxaluria | Double-blind randomised placebo-controlled trial. Oral Oxalobacter formigenes (107 colony forming units) twice daily for 24 weeks. Compliance self-reported. | 42 | 37/42 (88%) compliant. Overall vs. placebo, no significant change in mean UrOx (p = 0.62). Compliant vs. non-compliant UrOx not compared. | | 1995 | Leumann et al. [21] | Switzerland | Children with primary hyperoxaluria | Prospective interventional study with no controls. Oral sodium citrate (0.10-0.15 g/kg) daily, long term (mean 4 years). Compliance measured by variability in urinary pH and citrate load. | 7 | 3/5 (60%) compliant (other two lost to follow-up). Overall, significant decrease in mean UrOx (p = 0.02). Compliant vs. non-compliant UrOx not compared. | | 1991 | Edwards et al. [22] | UK | Adults with no disease, primary hyperoxaluria or mild metabolic hyperoxaluria | Prospective interventional study with healthy controls. Oral pyridoxine of various dosage. Compliance measured by urinary 4-pyridoxic acid. | 15 | 15/15 (100%) compliant. Compared to those with healthy patients, patients with mild metabolic hyperoxaluria, patients (p < 0.01) but not with primary hyperoxaluria displayed lower serum pyridoxal phosphate levels. No measurement of UrOx. No non-compliant patients for comparison. | | 1989 | D'Cruz et al. [23] | UK | Adults with enteric hyperoxaluria due to Crohn's disease+/-bowel resection | Prospective interventional study with no controls. Comparison of 24 h urine collection before and after 2 weeks of oral allopurinol 300 mg daily. Compliance measured by fall in plasma uric acid. | 8 | 8/8 (100%) patient compliant. Overall, no change in mean UrOx (p = n/s). No non-compliant patients for comparison. |
|
|
Eligible studies resulting from systematic review of intervention compliance among patients with hyperoxaluria.
|
| [1] |
B.H. Eisner, S. Sheth, S.P. Dretler, B. Herrick , V.M. Pais Jr.Abnormalities of 24-hour urine composition in first-time and recurrent stone-formers.Urology, 80(2012), pp. 776-779.
|
| [2] |
J.A. Prenen, P. Boer , E.J. Dorhout Mees.Absorption kinetics of oxalate from oxalate-rich food in man.Am J Clin Nutr, 40(1984), pp. 1007-1010.
|
| [3] |
G.E. von Unruh, S. Voss, T. Sauerbruch, A. Hesse.Reference range for gastrointestinal oxalate absorption measured with a standardized [13C2]oxalate absorption test.J Urol, 169(2003), pp. 687-690.
|
| [4] |
S. Voss, A. Hesse, D.J. Zimmermann, T. Sauerbruch ,G.E. von Unruh.Intestinal oxalate absorption is higher in idiopathic calcium oxalate stone formers than in healthy controls: measurements with the [(13)C2]oxalate absorption test.J Urol, 175(2006), pp. 1711-1715.
|
| [5] |
G.C. Curhan, W.C. Willett, E.B. Rimm , M.J. Stampfer. A prospective study of dietary calcium and other nutrients and the risk of symptomatic kidney stones.N Engl J Med, 328(1993), pp. 833-838.
|
| [6] |
L. Borghi, T. Schianchi, T. Meschi, A. Guerra, F. Allegri, U. Maggiore , et al.Comparison of two diets for the prevention of recurrent stones in idiopathic hypercalciuria.N Engl J Med, 346(2002), pp. 77-84.
|
| [7] |
S.A. Troxel, H. Sidhu, P. Kaul , R.K. Low.Intestinal Oxalobacter formigenes colonization in calcium oxalate stone formers and its relation to urinary oxalate.J Endourol, 17(2003), pp. 173-176.
|
| [8] |
R.W. Freel, M. Hatch, M. Green ,M. Soleimani.Ileal oxalate absorption and urinary oxalate excretion are enhanced in Slc26a6 null mice.Am J Physiol Gastrointest Liver Physiol, 290(2006), pp. G719-G728.
|
| [9] |
Z. Jiang, J.R. Asplin, A.P. Evan, V.M. Rajendran, H. Velazquez, T.P. Nottoli , et al.Calcium oxalate urolithiasis in mice lacking anion transporter Slc26a6.Nat Genet, 38(2006), pp. 474-478.
|
| [10] |
R.P. Holmes , D.G. Assimos.Glyoxylate synthesis, and its modulation and influence on oxalate synthesis.J Urol, 160(1998), pp. 1617-1624.
|
| [11] |
E.N. Taylor, M.J. Stampfer ,G.C. Curhan.Dietary factors and the risk of incident kidney stones in men: new insights after 14 years of follow-up.J Am Soc Nephrol, 15(2004), pp. 3225-3232.
|
| [12] |
M. Levine, C. Conry-Cantilena, Y. Wang, R.W. Welch, P.W. Washko, K.R. Dhariwal , et al.Vitamin C pharmacokinetics in healthy volunteers: evidence for a recommended dietary allowance.Proc Natl Acad Sci USA, 93(1996), pp. 3704-3709.
|
| [13] |
M. Menon ,C.J. Mahle.Oxalate metabolism and renal calculi.J Urol, 127(1982), pp. 148-151.
|
| [14] |
M.S. Krishnamurthy, K.A. Hruska ,P.S. Chandhoke. The urinary response to an oral oxalate load in recurrent calcium stone formers. J Urol, 169(2003), pp. 2030-2033
|
| 15 |
A. Trinchieri, F. Ostini, R. Nespoli, F. Rovera, G. Zanetti ,E. Pisani.. Hyperoxaluria in patients with idiopathic calcium nephrolithiasis. J Nephrol, 11(Suppl. 1) ( 1998), pp. 70-72.
|
| [16] |
A. Nouvenne, T. Meschi, A. Guerra, F. Allegri, B. Prati, E. Fiaccadori , et al.Diet to reduce mild hyperoxaluria in patients with idiopathic calcium oxalate stone formation: a pilot study.Urology, 73(2009), pp. 725-730.
|
| [17] |
L.K. Massey, H. Roman-Smith , R.A. Sutton.Effect of dietary oxalate and calcium on urinary oxalate and risk of formation of calcium oxalate kidney stones.J Am Diet Assoc, 93(1993), pp. 901-906.
|
| [18] |
A. Liberati, D.G. Altman, J. Tetzlaff, C. Mulrow, P.C. G?tzsche, J.P. Ioannidis, et al.The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol, 62(2009), pp. e1-34,http://doi.org/10.1371/journal.pmed.1000100 .
|
| [19] |
Z.R. Schwen, J.M. Riley, Y. Shilo ,T.D. Averch.Dietary management of idiopathic hyperoxaluria and the influence of patient characteristics and compliance.Urology, 82(2013), pp. 1220-1225.
|
| [20] |
B. Hoppe, J.W. Groothoff, S.A. Hulton, P. Cochat, P. Niaudet, M.J. Kemper , et al.Efficacy and safety of Oxalobacter formigenes to reduce urinary oxalate in primary hyperoxaluria.Nephrol Dial Transplant, 26(2011), pp. 3609-3615.
|
| [21] |
E. Leumann, B. Hoppe, T. Neuhaus ,N. Blau.Efficacy of oral citrate administration in primary hyperoxaluria.Nephrol Dial Transplant,10 (Suppl. 8) ( 1995), pp. 14-16.
|
| [22] |
P. Edwards , G.A. Rose. Metabolism of pyridoxine in mild metabolic hyperoxaluria and primary hyperoxaluria (type 1).Urol Int, 47(1991), pp. 113-117.
|
| [23] |
D.P. D'Cruz, D.J. Gertner, G.P. Kasidas, D.S. Rampton, G.A. Rose, C.T. Samuell.Failure of allopurinol to modify urinary composition in enteric hyperoxaluria.Br J Urol, 64(1989), pp. 231-234.
|
| [24] |
N.A. Laminski, A.M. Meyers, M. Kruger, M.I. Sonnekus , L.P. Margolius.Hyperoxaluria in patients with recurrent calcium oxalate calculi: dietary and other risk factors.Br J Urol, 68(1991), pp. 454-458.
|
| [25] |
K.L. Penniston , S.Y. Nakada.Effect of dietary changes on urinary oxalate excretion and calcium oxalate supersaturation in patients with hyperoxaluric stone formation.Urology, 73(2009), pp. 484-489.
|
| [26] |
J. Shuster, A. Jenkins, C. Logan, T. Barnett, R. Riehle, D. Zackson , et al.Soft drink consumption and urinary stone recurrence: a randomized prevention trial.J Clin Epidemiol, 45(1992), pp. 911-916.
|
| [27] |
L. Borghi, T. Meschi, F. Amato, A. Briganti, A. Novarini , A. Giannini.Urinary volume, water and recurrences in idiopathic calcium nephrolithiasis: a 5-year randomized prospective study.J Urol, 155(1996), pp. 839-843.
|
| [28] |
K. Sarica, Y. Inal, S. Erturhan ,F. Ya?ci.The effect of calcium channel blockers on stone regrowth and recurrence after shock wave lithotripsy.Urol Res, 34(2006), pp. 184-189.
|
| [29] |
R.P. Holmes, H.O. Goodman , D.G. Assimos.Contribution of dietary oxalate to urinary oxalate excretion.Kidney Int, 59(2001), pp. 270-276.
|
| [30] |
L.K. Massey, M. Liebman , S.A. Kynast-Gales.Ascorbate increases human oxaluria and kidney stone risk.J Nutr, 135(2005), pp. 1673-1677.
|
| [31] |
S. Baddar, B. Jayakrishnan ,O.A. Al-Rawas.Asthma control: importance of compliance and inhaler technique assessments.J Asthma, 51(2014), pp. 429-434.
|
| [32] |
E. Kuyucu, F. Ko?yi?it , L. Cift?i.The importance of patient compliance in nonunion of forearm fracture.Int J Surg Case Rep, 5(2014), pp. 598-600.
|
| [33] |
K. Bensalah, A. Tuncel, J.D. Raman, A. Bagrodia, M. Pearle ,Y. Lotan.How physician and patient perceptions differ regarding medical management of stone disease.J Urol, 182(2009), pp. 998-1004.
|
| [34] |
C. Kwak, H.K. Kim, E.C. Kim, M.S. Choi , H.H. Kim.Urinary oxalate levels and the enteric bacterium Oxalobacter formigenes in patients with calcium oxalate urolithiasis.Eur Urol, 44(2003), pp. 475-481.
|
| [35] |
R. Siener, D. Ebert ,A. Hesse.Urinary oxalate excretion in female calcium oxalate stone formers with and without a history of recurrent urinary tract infections.Urol Res, 29(2001), pp. 245-248.
|
| [36] |
J.P. Kelly, G.C. Curhan, D.R. Cave, T.E. Anderson , D.W. Kaufman.Factors related to colonization with Oxalobacter formigenes in U.S. adults.J Endourol, 25(2011), pp. 673-679.
|
| [37] |
E. Lee, B.C. Jeong, Y.H. Park , H.H. Kim.Expression of the gene encoding oxalate decarboxylase from Bacillus subtilis and characterization of the recombinant enzyme.BMC Res Notes, 7(2014), p. 598.
|
| [38] |
P.K. Poonguzhali ,H. Chegu.The influence of banana stem extract on urinary risk factors for stones in normal and hyperoxaluric rats.Br J Urol, 74(1994), pp. 23-25.
|
| [39] |
N. Saravanan, D. Senthil ,P. Varalakshmi. Effect of L-cysteine on some urinary risk factors in experimental hyperoxaluric rats. Br J Urol, 78(1996), pp. 22-24.
|
| [40] |
M. Adhirai ,R. Selvam. Effect of cyclosporin on liver antioxidants and the protective role of vitamin E in hyperoxaluria in rats.J Pharm Pharmacol, 50(1998), pp. 501-505.
|
| [1] |
Russell S. Terry,Glenn M. Preminger. Metabolic evaluation and medical management of staghorn calculi[J]. Asian Journal of Urology, 2020, 7(2): 122-129. |
| [2] |
Osman Ermis,Bhaskar Somani,Thomas Reeves,Selcuk Guven,Pilar Laguna Pes,Arun Chawla,Padmaraj Hegde,Jean de la Rosette. Definition, treatment and outcome of residual fragments in staghorn stones[J]. Asian Journal of Urology, 2020, 7(2): 116-121. |
| [3] |
Nariman Gadzhiev,Vigen Malkhasyan,Gagik Akopyan,Sergei Petrov,Francis Jefferson,Zhamshid Okhunov. Percutaneous nephrolithotomy for staghorn calculi: Troubleshooting and managing complications[J]. Asian Journal of Urology, 2020, 7(2): 139-148. |
| [4] |
Bohdan Baralo,Patrick Samson,David Hoenig,Arthur Smith. Percutaneous kidney stone surgery and radiation exposure: A review[J]. Asian Journal of Urology, 2020, 7(1): 10-17. |
| [5] |
Liu Yu,Chen Yuntian,Liao Banghua,Luo Deyi,Wang Kunjie,Li Hong,Zeng Guohua. Epidemiology of urolithiasis in Asia[J]. Asian Journal of Urology, 2018, 5(4): 205-214. |
| [6] |
Carter Boyd,Kyle Wood,Dustin Whitaker,Dean G. Assimos. The influence of metabolic syndrome and its components on the development of nephrolithiasis[J]. Asian Journal of Urology, 2018, 5(4): 215-222. |
| [7] |
Jennifer Bjazevic,Hassan Razvi*. Stones in pregnancy and pediatrics[J]. Asian Journal of Urology, 2018, 5(4): 223-234. |
| [8] |
Matthias Beysens,Thomas O. Tailly. Ureteral stents in urolithiasis[J]. Asian Journal of Urology, 2018, 5(4): 274-286. |
| [9] |
Daniel A. Wollin,Adam G. Kaplan,Glenn M. Preminger,Pietro Manuel Ferraro,Antonio Nouvenne,Andrea Tasca,Emanuele Croppi,Giovanni Gambaro,Ita P. Heilberg. Defining metabolic activity of nephrolithiasis - Appropriate evaluation and follow-up of stone formers[J]. Asian Journal of Urology, 2018, 5(4): 235-242. |
| [10] |
Luke F. Reynolds,Tad Kroczak,Kenneth T. Pace. Indications and contraindications for shock wave lithotripsy and how to improve outcomes[J]. Asian Journal of Urology, 2018, 5(4): 256-263. |
| [11] |
María Rodríguez-Monsalve Herrero,Steeve Doizi,Etienne Xavier Keller,Vincent De Coninck,Olivier Traxer. Retrograde intrarenal surgery: An expanding role in treatment of urolithiasis[J]. Asian Journal of Urology, 2018, 5(4): 264-273. |
| [12] |
Hung Jung Jae,Park Jinsung,Tae Kim Won,WookKim Hong,JoonKim Hyung,Hong Sungwoo,JoYang Hee,Chung Hong. The association of benign prostatic hyperplasia with lower urinary tract stones in adult men: A retrospective multicenter study[J]. Asian Journal of Urology, 2018, 5(2): 118-121. |
| [13] |
Vinaya Vasudevan, Patrick Samson, Arthur D. Smith, Zeph Okeke. The genetic framework for development of nephrolithiasis[J]. Asian Journal of Urology, 2017, 4(1): 18-26. |
| [14] |
Husain Alenezi, John D. Denstedt. Flexible ureteroscopy: Technological advancements, current indications and outcomes in the treatment of urolithiasis[J]. Asian Journal of Urology, 2015, 2(3): 133-141. |
|
|
|
|