|
|
|
| The role of radiotherapy in localised and locally advanced prostate cancer |
Michel Bollaa,*( ),Ann Henryb,Malcom Masonc,Thomas Wiegeld ),Ann Henryb,Malcom Masonc,Thomas Wiegeld
|
a. Department of Radiation Oncology, Grenoble Alpes University, Grenoble, France;
b. Department of Clinical Oncology, St. James's University Hospital, Leeds, UK;
c.Cardiff University, Velindre Hospital, Whitchurch, UK;
d.Department of Radiation Oncology, University Hospital Ulm, Germany |
|
|
|
|
Abstract For a patient suffering from non-metastatic prostate cancer, the individualized recommendation of radiotherapy has to be the fruit of a multidisciplinary approach in the context of a Tumor Board, to be explained carefully to the patient to obtain his informed consent. External beam radiotherapy is now delivered by intensity modulated radiotherapy, considered as the gold standard. From a radiotherapy perspective, low-risk localized prostate cancer is treated by image guided intensity modulated radiotherapy, or brachytherapy if patients meet the required eligibility criteria. Intermediate-risk patients may benefit from intensity modulated radiotherapy combined with 4-6 months of androgen deprivation therapy; intensity modulated radiotherapy alone or combined with brachytherapy can be offered to patients unsuitable for androgen deprivation therapy due to co-morbidities or unwilling to accept it to preserve their sexual health. High-risk prostate cancer, i.e. high-risk localized and locally advanced prostate cancer, requires intensity modulated radiotherapy with long-term (≥2 years) androgen deprivation therapy with luteinizing hormone releasing hormone agonists. Post-operative irradiation, either immediate or early deferred, is proposed to patients classified as pT3pN0, based on surgical margins, prostate-specific antigen values and quality of life. Whatever the techniques and their degree of sophistication, quality assurance plays a major role in the management of radiotherapy, requiring the involvement of physicians, physicists, dosimetrists, radiation technologists and computer scientists. The patients must be informed about the potential morbidity of radiotherapy and androgen deprivation therapy and followed regularly during and after treatment for tertiary prevention and evaluation. A close cooperation is needed with general practitioners and specialists to prevent and mitigate side effects and maintain quality of life.
|
|
Received: 16 October 2018
Available online: 08 February 2019
|
|
Corresponding Authors:
Michel Bolla
E-mail: MBolla@chu-grenoble.fr
|
|
|
|
|
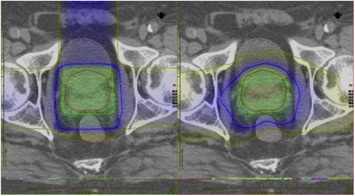
Dose distributions for intensity-modulated radiotherapy (IMRT) (right) and standard, conformal radiotherapy (left) to the prostate. Note the improved dose distribution and concave high dose volume with IMRT. Courtesy of Dr Gareth Jones, Velindre Hospital, Cardiff.
|

| Study/Author | n | Risk, GS, or NCCN | ADT | RT regimen | BED, Gy | Median FU, month | Outcome | | Lee et al. [9] | 550
542 | low risk | None | 70 Gy/28 fx
73.8 Gy/41 fx | 80
69.6 | 70 | 5 year DFS 86.3% (n.s.)
5 year DFS 85.3% | | Dearnaley et al. [10] | 1077/19 fx
1074/20 fx
1065/37 fx | 15% low
73% intermediate
12% high | 3-6 months, before and during EBRT | 57 Gy/19 fx
60 Gy/20 fx
74 Gy/37 fx | 73.3
77.1
74 | 62 | 5 year BCDF
85.9% (19 fx)
90.6% (20 fx)
88.3% (37 fx) | | Aluwini et al. [6] | 403
392 | 30% GS <6, 45% GS >7, 25% GS 8-10 | None | 64.6 Gy/19 fx
78 Gy/39 fx | 90.4
78 | 60 | 5 year RFS 80.5% (n.s.)
5 year RFS 77.1% | | Catton et al. [11] | 608 | intermediate risk
53% T1c
46% T2a-c | None | 60 Gy/20 fx | 77.1 | 72 | 5 year BCDF
both arms 85%
HR: 0.96 (n.s) | | 598 | 9% GS 6
63% GS 7a
28% GS 7b | 78 Gy/39 fx | 78 |
|
|
Major phase III randomised trials of moderate hypofractionation for primary treatment.
|
| Comparison of prostate brachytherapy techniques | | LDR | ?
Permanent seeds implanted at single visit
?
Uses Iodine-125 (most common), Palladium-103 or Caesium-131 isotopes
?
Radiation dose delivered over weeks and months
?
Acute side effects resolve over months
?
Radiation protection issues for patient and carers
?
shielded theatre room
?
Established as monotherapy for low and selected intermediate risk localized prostate cancer
?
Established as a boost treatment with external beam radiation in higher risk or locally advanced prostate cancer | | HDR | ?
Temporary implantation and may need to be fractionated
?
Ir-192 (most common) Co-60 source introduced through implanted applicators (needles or catheters)
?
Radiation dose delivered in minutes
?
Acute side effects resolve over weeks
?
No radiation protection issues for patient or carers
?
Can use same HDR source for other cancer treatments
?
Need for a shielded HDR treatment room
?
Established as boost treatment with external beam radiation in higher risk or locally advanced prostate cancer
?
Single centre cohort studies demonstrate good outcomes when used as monotherapy for localised disease |
|
|
Comparison of prostate brachytherapy techniques.
|
| Trial | Year | TNM stage | n | Trial | ADT | RT | Effect on OS | | EORTC 22863 [31] | 2010 | T1-2 poorly differentiated
and M0, or T3-4 N0-1 M0 | 415 | EBRT ± ADT | LHRHa for 3 years (adjuvant) | 70 Gy RT | Benefit at 10-year for combined treatment (p = 0.0004) | | RTOG 85-31 [32] | 2005 | T3 or N1 M0 (15% RP) | 977 | EBRT ± ADT | Orchiectomy
or LHRHa | 65-70 Gy RT | Benefit for combined treatment (p = 0.002) mostly caused by patients with Gleason score 7-10 | | D'Amico [7], [8], [9], [10] | 2008 | T2 N0 M0 (localised unfavourable
risk) | 206 | EBRT ± ADT | LHRHa plus flutamide
for 6 mo. | 70 Gy
3D-CRT | Significant benefit (p = 0.01) that may pertain only to men with no or minimal comorbidity | | TROG 96-01 [39] | 2011 | T2b-4 N0 M0 | 802 | Neoadjuvant
ADT duration | LHRHa plus flutamide 3 or 6 mo.
before, plus concomitant | 66 Gy
3D-CRT | Benefit in PCa-specific survival (p = 0.04) | | RTOG 94-13 [40] | 2007 | T1c-4 N0-1 M0 | 1292 | ADT timing comparison | 2 mo. neoadjuvant
plus concomitant
vs. 4 mo.
adjuvant | Whole pelvic RT vs.
prostate only;
70.2 Gy | No significant difference between neoadjuvant plus concomitant vs. adjuvant
androgen suppression
therapy groups (interaction suspected) | | RTOG 86-10 [38] | 2008 | T2-4 N0-1 | 456 | EBRT ± ADT | LHRHa plus flutamide
2 mo. before, plus concomitant | 65-70 Gy RT | No significant difference at 10 year | | RTOG 92-02 [33] | 2008 | T2c-4 N0-1 M0 | 1554 | Short vs. prolonged
ADT | LHRHa given for 2 years as adjuvant after 4 mo. as neoadjuvant | 65-70 Gy RT | 10-year OS benefit in subset with Gleason 8-10 for long-term ADT (p = 0.006) | | EORTC 22961 [34] | 2009 | T1c-2ab N1
M0, T2c-4
N0-1 M0 | 970 | Short vs. prolonged
ADT | LHRHa for 6 mo. vs.
3 years | 70 Gy
3D-CRT | Better 5-year OS with 3-year treatment (p = 0.006) | | SPCG-7/SFUO-3 [35] | 2014 | T1b-2 Grade
2-3, T3 N0 M0 | 875 | ADT ± EBRT | LHRH a for 3 mo plus continuous
flutamide | 70 Gy
3D-CRT vs. no RT | Lower 15-year cancer specific mortality (30.7%) vs. (12.4%) favouring combined treatment (p < 0.0001) | | NCIC CTGMRC/PR3/PRO7/SWOG [36] | 2015 | T3-4 (88%),
PSA >20 ng/mL (64%), GS 8-10 (36%) N0 M0 | 1205 | ADT ± EBRT | Continuous
LHRHa | 65-70 Gy
3D-CRT vs. no RT | 10-year OS benefit for combined treatment (p < 0.001) | | French study [37] | 2012 | T3-4 N0 M0 | 273 | ADT ± EBRT | LHRHa for 3 year | 70 Gy
3D-CRT vs. no RT | Better 5-year progression free survival for combined treatment (p < 0.001) | | 264 |
|
|
Major phase III randomized trials of use and duration of ADT in combination with RT for PCa.
|
| [1] |
N. Mottet, J. Bellmunt, M. Bolla, E. Briers, M.G. Cumberbatch, S. De Santis , et al.Members of the EAU-ESTRO-ESUR-SIOG. Guidelines panel on prostate cancer.(2017).http://uroweb.org/guideline/prostate-cancer/ .
|
| [2] |
A. Kalbasi, J. Li, A. Berman , S. Swisher-McClure, M. Smaldone, R.G. Uzzo, et al.Dose escalated irradiation and overall survival in men with nonmetastatic prostate cancer.JAMA Oncol, 1(2015), pp. 897-906.
doi: 10.1016/j.juro.2015.12.018
pmid: 26181727
|
| [3] |
F.C. Hamdy, J.L. Donovan, J.A. Lane, M. Mason, C. Metcalfe, P. Holding , et al.10-year outcomes after monitoring, surgery, or radiotherapy for localized prostate cancer.N Engl J Med, 375(2016), pp. 1415-1424.
|
| [4] |
J.F. Fowler, I. Toma-Dasu , A. et Dasu.Is the α/β ratio for prostate tumours really low and does it vary with the level of risk at diagnosis?. Anticancer Res, 33(2013), pp. 1009-1011
pmid: 23482774
|
| [5] |
B.F. Koontz, A. Bossi, C. Cozzarini, T. Wiegel , A. D'Amico.A Systematic review of hypofractionation for primary management of prostate cancer.Eur Urol, 68(2015), pp. 683-691.
doi: 10.1016/j.eururo.2014.08.009
pmid: 25171903
|
| [6] |
S. Aluwini, F. Pos, E. Schimmel, S. Krol , P.P. van der Toorn, H. de Jager, et al.Hypofractionated versus conventionally fractionated radiotherapy for patients with prostate cancer (HYPRO): late toxicity results from a randomised, non-inferiority, phase 3 trial.Lancet Oncol, 17(2016), pp. 464-474.
|
| [7] |
C.E. Vargas, W.F. Hartsell, M. Dunn, S.R. Keole, L. Doh, E. Eisenbeisz , et al.Hypofractionated versus standard fractionated proton-beam therapy for low-risk prostate cancer: interim results of a randomized trial PCG GU 002.Am J Clin Oncol, 41(2015), pp. 115-12.
doi: 10.1016/j.ijrobp.2015.07.474
pmid: 26523442
|
| [8] |
A. Wilkins, H. Mossop, I. Syndikus, V. Khoo, D. Bloomfield, C. Parker , et al.Hypofractionated radiotherapy versus conventionally fractionated radiotherapy for patients with intermediate-risk localised prostate cancer: 2-year patient-reported outcomes of the randomised, non-inferiority, phase 3 CHHiP trial.Lancet Oncol, 16(2015), pp. 1605-1616.
doi: 10.1016/S1470-2045(15)00280-6
pmid: 4664817
|
| [9] |
W.R. Lee, J.J. Dignam, M.B. Amin, D.W. Bruner, D. Low, G.P. Swanson , et al.Randomized phase III noninferiority study comparing two radiotherapy fractionation schedules in patients with low-risk prostate cancer.J Clin Oncol, 34(2016), pp. 2325-2332.
doi: 10.1200/JCO.2016.67.0448
pmid: 27044935
|
| [10] |
D. Dearnaley, I. Syndikus, H. Mossop, V. Khoo, A. Birtle, D. Bloomfield , et al.Conventional versus hypofractionated high-dose intensity-modulated radiotherapy for prostate cancer: 5-year outcomes of the randomised, non-inferiority, phase 3 CHHiP trial.Lancet Oncol, 17(2016), pp. 1047-1060.
doi: 10.1016/S1470-2045(16)30102-4
pmid: 4961874
|
| [11] |
C.N. Catton, H. Lukka, C.S. Gu, J.M. Martin, S. Supiot , P.W.M. Chung, et al.Randomized trial of a hypofractionated radiation regimen for the treatment of localized prostate cancer.J Clin Oncol, 35(2017), pp. 1884-1890.
|
| [12] |
D.R. Henderson, A.C. Tree , N.J. van As.Stereotactic body radiotherapy for prostate cancer.Clin Oncol (R Coll Radiol), 27(2015), pp. 270-279.
doi: 10.1016/j.clon.2015.01.011
pmid: 25707911
|
| [13] |
N.G. Zaorsky, N. Ohri, T.N. Showalter, A.P. Dicker , R.B. Den.Systematic review of hypofractionated radiation therapy for prostate cancer.Cancer Treat Rev, 39(2013), pp. 728-736.
doi: 10.1016/j.ctrv.2013.01.008
pmid: 3833592
|
| [14] |
A.J. Katz , J. Kang.Stereotactic body radiotherapy as treatment for organ confined low- and intermediate-risk prostate carcinoma, a 7-year study.Front Oncol, 4(2014), p. 240.
doi: 10.3389/fonc.2014.00240
pmid: 25229051
|
| [15] |
C. Salembier, P. Lavagnini, P. Nickers, P. Mangili, A. Rijnders, A. Polo , et al.Tumour and target volumes in permanent prostate brachytherapy: a supplement to the ESTRO/EAU/EORTC recommendations on prostate brachytherapy.Radiother Oncol, 83(2007), pp. 3-10.
doi: 10.1016/j.radonc.2007.01.014
pmid: 17321620
|
| [16] |
P.J. Hoskin, A. Colombo, A. Henry, P. Niehoff, T. Paulsen Hellebust, F.A. Siebert , et al.GEC/ESTRO recommendations on high dose rate afterloading brachytherapy for localised prostate cancer: an update.Radiother Oncol, 107(2013), pp. 325-332.
doi: 10.1016/j.radonc.2013.05.002
pmid: 23773409
|
| [17] |
D.Y. Gelblum, L. Potters, R. Ashley, R. Waldbaum, X.H. Wang, S. Leibel , et al.Urinary morbidity following ultra-sound guided transperineal prostate seed implantation.Int J Radiat Oncol Biol Phys, 45(1999), pp. 59-67.
doi: 10.1016/S0360-3016(99)00176-5
pmid: 10477007
|
| [18] |
C. Martens, G. Pond, D. Webster, M. McLean, C. Gillan , J. Crook.Relationship of the International Prostate Symptom Score with urinary flow studies and catheterization rates following 125I prostate brachytherapy.Brachytherapy , 5(2006), pp. 9-13.
doi: 10.1016/j.brachy.2005.12.002
pmid: 16563992
|
| [19] |
J. Chin, R.B. Rumble, M. Kollmeier, E. Heath, J. Efstathiou, T. Dorff , et al.Brachytherapy for patients with prostate cancer: American society of clinical oncology/cancer care Ontario joint guideline update.J Clin Oncol, 35(2017), pp. 1737-1743.
doi: 10.1200/JCO.2016.72.0466
pmid: 28346805
|
| [20] |
W.J. Morris, S. Tyldesley, S. Rodda, R. Halperin, H. Pai, M. McKenzie , et al.Androgen suppression Combined with elective nodal and dose escalated radiation therapy (the ASCENDE-RT Trial): an analysis of survival endpoints for a randomized trial comparing a low-dose-rate brachytherapy boost to a dose-escalated external beam boost for high- and intermediate-risk prostate cancer.Int J Radiat Oncol Biol Phys, 98(2017), pp. 275-285.
|
| [21] |
N. Tselis, P. Hoskin, D. Baltas, V. Strnad, N. Zamboglou, C. R?del , et al.High dose rate brachytherapy as monotherapy for localised prostate cancer: review of the current status.Clin Oncol, 29(2017), pp. 401-411.
doi: 10.1016/j.clon.2017.02.015
pmid: 29074079
|
| [22] |
I.M. Thompson, C.M. Tangen, J. Paradelo, M.S. Lucia, G. Miller, D. Troyer , et al.Adjuvant radiotherapy for pathological T3N0M0 prostate cancer significantly reduces risk of metastases and improves survival: long-term followup of a randomized clinical trial.J Urol, 181(2009), pp. 956-962.
doi: 10.1016/j.juro.2008.11.032
pmid: 3510761
|
| [23] |
M. Bolla , H. van Poppel, B. Tombal, K. Vekemans, L. Da Pozzo, T.M. de Reijke, et al.Postoperative radiotherapy after radical prostatectomy for high-risk prostate cancer: long-term results of a randomised controlled trial (EORTC trial 22911).Lancet, 380(2012), pp. 2018-2027.
doi: 10.1016/s0140-6736(12)61253-7
|
| [24] |
T. Wiegel, D. Bartkowiak, D. Bottke, C. Bronner, U. Steiner, A. Siegmann , et al.Adjuvant radiotherapy versus wait-and-see after radical prostatectomy: 10-year follow-up of the ARO 96-02/AUO AP 09/95 trial.Eur Urol, 66(2014), pp. 243-250.
doi: 10.1016/j.eururo.2014.03.011
pmid: 24680359
|
| [25] |
T. Wiegel , LohmG, D. Bottke, S. H?cht, K. Miller, A. Siegmann, et al.Achieving an undetectable PSA after radiotherapy for biochemical progression afetr radical prostatectomy is an independant predictor of biochemical outcome—results of a retrospective study.Int J Radiat Oncol Biol Phys, 73(2009), pp. 1009-1016.
doi: 10.1016/j.ijrobp.2008.06.1922
pmid: 18963539
|
| [26] |
A.J. Stephenson, P.T. Scardino, M.W. Kattan, T.M. Pisansky, K.M. Slawin, E.A. Klein , et al.Predicting the outcome of salvage radiation therapy for reccurent prostate cancer after radical prostatectomy.J Clin Oncol, 25(2007), pp. 2035-2041.
|
| [27] |
C.R. King.The timing of salavge radiotherapy after radical prostatectomy: a systematic review.Int J Radiat Oncol Biol Phys, 84(2012), pp. 104-111.
|
| [28] |
P. Ghadjar, S. Hayoz, J. Bernhard, D.R. Zwahlen, T. Holscher, P. Gut , et al.Acute toxicity and quality of life after dose-intensified salvage radiation therapy for biochemically recurrent prostate cancer after prostatectomy: first results of the randomized trial SAKK 09/10.J Clin Oncol, 33(2015), pp. 4158-4166
doi: 10.1200/JCO.2015.63.3529
pmid: 26527774
|
| [29] |
C. Carrie, A. Hasbini , G. de Laroche, P. Richaud, S. Guerif, I. Latorzeff, et al.Salvage radiotherapy with or without short-term hormone therapy for rising prostate-specific antigen concentration after radical prostatectomy (GETUG-AFU 16): a randomised, multicentre, open-label phase 3 trial.Lancet Oncol, 17(2016), pp. 747-756.
doi: 10.1016/S1470-2045(16)00111-X
pmid: 27160475
|
| [30] |
W.U. Shipley, W. Seiferheld, H.R. Lukka, P.P. Major, N.M. Heney, D.J. Grignon , et al.Radiation with or without antiandrogen therapy in recurrent prostate cancer.N Engl J Med, 376(2017), pp. 417-428.
doi: 10.1056/NEJMoa1607529
pmid: 28146658
|
| [31] |
A. Briganti, T. Wiegel, S. Joniau, C. Cozzarini, M. Bianchi, M. Sun , et al.Early salvage radiation therapy does not compromise cancer control in patients with pT3N0 prostate cancer after radical prostatectomy : results of a matche-controlled multi-institutional analysis.Eur Urol, 62(2012), pp. 472-487.
doi: 10.1016/j.eururo.2012.04.056
pmid: 22633803
|
| [32] |
M. Bolla , G. van Tienhoven, P. Warde, J.B. Dubois, R.O. Mirimanoff, G. Storme, et al.External irradiation with or without long-term androgen suppression for prostate cancer with high metastatic risk: 10-year results of an EORTC randmized study.Lancet Oncol, 11(2010), pp. 1066-1073.
doi: 10.1016/S1470-2045(10)70223-0
pmid: 20933466
|
| [33] |
M.V. Pilepich, K. Winter, C.A. Lawton, R.E. Krisch, H.B. Wolkov, B. Movsas , et al.Androgen suppression adjuvant to definitive radiotherapy in prostate carcinoma-long-term results of phase III RTOG 85-31.Int J Radiat Oncol Biol Phys, 61(2005), pp. 1285-1290.
doi: 10.1016/j.ijrobp.2004.08.047
pmid: 15817329
|
| [34] |
E.M. Horwitz, K. Bae, G.E. Hanks, A. Porter, D.J. Grignon, H.D. Brereton , et al.Ten-year follow-up of radiation therapy oncology group protocol 92-02: a phase III trial of the duration of elective androgen deprivation in locally advanced prostate cancer.J Clin Oncol, 26(2008), pp. 2497-2504.
doi: 10.1200/JCO.2007.14.9021
pmid: 18413638
|
| [35] |
M. Bolla , T.M. de Reijke, G. Van Tienhoven, A.C. Van den Bergh, J. Oddens, P.M. Poortmans, et al.Duration of androgen suppression in the treatment of prostate cancer.N Engl J Med, 360(2009), pp. 2516-2527.
|
|
S.D. Fossa, F. Wiklund, O. Klepp, A. Angelsen, A. Solberg, J.E. Damber , et al.Ten- and 15-year prostate cancer-specific mortality in patients with non metastatic locally advanced or aggressive intermediate prostate cancer, randomized to lifelong endocrine treatment alone or combined with radiotherapy; final results of the Scandinavian Prostate Cancer Group-7.Eur Urol, 70(2016), pp. 684-691.
|
| [37] |
M. Mason, W.R. Parulekar, M.R. Sydes, M. Brundage, P. Kirkbride, M. Gospodarowicz , et al.Final report of the intergroup randomized study of combined androgen deprivationtherapy plus radiotherapy versus androgen deprivation therapy alone in locally advanced prostate cancer.J Clin Oncol, 33(2015), pp. 2143-2150.
|
| [38] |
N. Mottet, M. Peneau, J.J. Mazeron, V. Molinie , P. Richaud.Addition of radiotherapy to long term androgen deprivation in locally advanced prostate cancer: an open randomised phase 3 trial.Eur Urol, 62(2012), pp. 213-219.
doi: 10.1016/j.eururo.2012.03.053
pmid: 22502942
|
| [39] |
M. Roach 3rd, K. Bae, J. Speight, H.B. Wolkov, P. Rubin, R.J. Lee, et al.Short-term neoadjuvant androgen deprivation therapy and external-beam radiotherapy for locally advanced prostate cancer: long-term results of RTOG 86-10.J Clin Oncol, 26(2008), pp. 585-591.
doi: 10.1200/JCO.2007.13.9881
pmid: 18172188
|
| [40] |
J.W. Denham, A. Steigler, D.S. Lamb, D. Joseph, S. Turner, J. Matthews , et al.Short term neoadjuvant androgen deprivation and radiotherapy for locally advanced prostate cancer: 10-year data from the TROG 96.01 randomised trial.Lancet Oncol, 12(2011), pp. 451-459.
doi: 10.1016/S1470-2045(11)70063-8
pmid: 21440505
|
| [41] |
C.A. Lawton, M. DeSivio , M. Roach 3rd, V. Uhl, R. Kirsch, M. Seider, et al.An update of the phase III trial comparing whole pelvis to prostate only radiotherapy and neoadjuvant to adjuvant total androgen suppression.: update analysis of RTOG 94-13, with emphasis on unexpected hormone/radiation interactions.Int J Radiat Oncol Biol Phys, 69(2007), pp. 646-655.
|
| [42] |
C.A. Lawton, K. Winter, D. Grignon , M.V. Pilepich.Androgen suppression plus radiation versus radiation alone for patients with D1/pathologic node-positive adenocarcinoma of the prostate: updated results based on a national prospective randomized trial, Radiation Therapy Oncology Group 85-31.Int J Radiat Oncol Biol Phys, 23(2005), pp. 800-807.
doi: 10.1200/jco.2005.08.141
pmid: 15681524
|
| [43] |
A. Briganti, R.J. Karnes , L.F. Da Pozzo, C. Cozzarini, U. Capitanio, A. Gallina, et al.Combination of adjuvant hormonal and radiation therapy significantly prolongs survival of patients with pT2-4 pN+ prostate cancer: results of a matched analysis.Eur Urol, 59(2011), pp. 832-840.
doi: 10.1016/j.eururo.2011.02.024
pmid: 21354694
|
| [44] |
C.C. Lin, P.J. Gray, A. Jemal , J.A. EfstathiouAndrogen deprivation with or without radiation therapy for clinically node-positive prostate cancer. J Natl Cancer Inst, 107(2015), pp. 1-10.
doi: 10.1093/jnci/djv119
pmid: 25957435
|
| [45] |
N.D. James, M.R. Spears, N.W. Clarke, D.P. Dearnaley, M.D. Mason, C.C. Parker , et al.Failure-free survival and radiotherapy in patients with newly diagnosed nonmetastatic prostate cancer: data from patients in the control arm of the STAMPEDE trial.JAMA Oncol, 2(2016), pp. 348-357.
doi: 10.1001/jamaoncol.2015.4350
pmid: 26606329
|
| [46] |
A.L. Potosky, K. Knopf, L.X. Clegg, P.C. Albertsen, J.L. Stanford, A.S. Hamilton , et al.Quality-of-life outcomes after primary androgen deprivation therapy: results from the Prostate Cancer Outcomes Study.J Clin Oncol, 19(2001), pp. 3750-3757.
doi: 10.1007/s004320100259
pmid: 11533098
|
| [47] |
J.A. Efstathiou, K. Bae, W.U. Shipley, G.E. Hanks, M.V. Pilepich, H.M. Sandler , et al.Cardiovascular mortality and duration of androgen deprivation for locally advanced prostate cancer: analysis of RTOG 92-02.Eur Urol, 54(2008), pp. 816-823.
doi: 10.1016/j.eururo.2008.01.021
pmid: 18243509
|
| [48] |
J.A. Efstathiou, K. Bae, W.U. Shipley, G.E. Hanks, M.V. Pilepich, H.M. Sandler , et al.Cardiovascular mortality after androgen deprivation therapy for locally advanced prostate cancer: RTOG 85-31.J Clin Oncol, 27(2009), pp. 92-99.
doi: 10.1200/JCO.2007.12.3752
pmid: 2645096
|
| [49] |
M.R. Smith, K. Bae, J.A. Efstathiou, G.E. Hanks, M.V. Pilepich, H.M. Sandler , et al.Diabetes and mortality in men with locally advanced prostate cancer.J Clin Oncol, 26(2008), pp. 4333-4339.
|
| [50] |
M.R. Smith, B. Egerdie, N. Hernandez Toriz, R. Feldman, T.L. Tammela, F. Saad , et al.Denosumab in men receiving androgen-deprivation therapy for prostate cancer.N Engl J Med, 361(2009), pp. 745-755.
|
| No related articles found! |
|
|
|
|