|
|
|
| The impact of urological resection and reconstruction on patients undergoing cytoreductive surgery (CRS) and hyperthermic intraperitoneal chemotherapy (HIPEC) |
Grace Hwei ChingTana,Nicholas B.Shannonb,Claramae ShulynChiaa,Lui ShiongLeec,Khee CheeSooa,Melissa Ching Ching Teoa*( ) )
|
a Division of Surgical Oncology, National Cancer Centre Singapore, Singapore
b Duke-NUS Medical School, Singapore
c Department of Urology, Singapore General Hospital, Singapore |
|
|
|
|
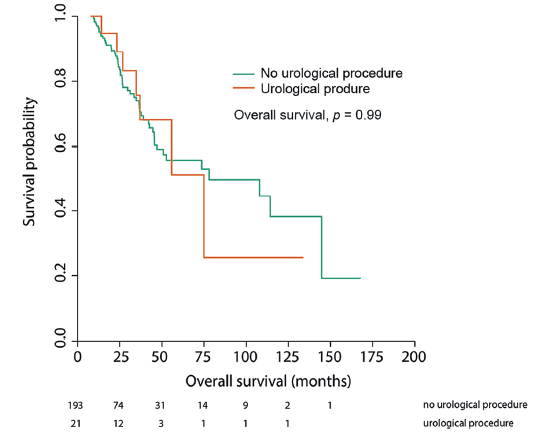
Abstract Objective: Cytoreductive surgery (CRS) and hyperthermic intraperitoneal chemotherapy (HIPEC) are increasingly being used to treat peritoneal malignancies. Urological resections and reconstruction (URR) are occasionally performed during the surgery. We aim to evaluate the impact of these procedures on peri-operative outcomes of CRS and HIPEC patients. Methods: A retrospective review of a prospectively maintained database of all patients who underwent CRS-HIPEC from April 2001 to February 2016 was performed. Outcomes between patients who had surgery involving, and not involving URR were compared. Primary outcomes were the rate of major complications and the duration of stay in the intensive care unit (ICU) and hospital. Secondary outcomes were that of overall survival (OS) and prognostic factors that would indicate a need for URR. Results: A total of 214 CRS-HIPEC were performed, 21 of which involved a URR. Baseline clinical characteristics did not vary between the groups (URR vs. No URR). Urological resections comprised of 52% bladder resections, 24% ureteric resections, and 24% involving both bladder and ureteric resections. All bladder defects were closed primarily while ureteric reconstructions consisted of two end-to-end anastomoses, one ureto-uretostomy, five direct implantations into the bladder and three boari flaps. URR were more frequently required in patients with colorectal peritoneal disease (p = 0.029), but was not associated with previous pelvic surgery (76% vs. 54%, p = 0.065). Patients with URR did not suffer more serious complications (14% vs. 24%, p = 0.42). ICU (2.2 days vs. 1.4 days, p = 0.51) and hospital stays (18 days vs. 25 days, p = 0.094) were not significantly affected. Undergoing a URR did not affect OS (p = 0.99), but was associated with increased operation time (570 min vs. 490 min, p = 0.046). Conclusion: While concomitant URR were associated with an increase in operation time, there were no significant differences in postoperative complications or OS. Patients with colorectal peritoneal metastases are more likely to require a URR compared to other primary tumours, and needs to be considered during pre-operative planning.
|
|
Received: 09 September 2016
Published: 23 July 2018
|
|
Corresponding Authors:
Ching Ching Teo Melissa
E-mail: Melissa.Teo.C.C@nccs.com.sg
|
|
|

| Any urological procedure | n (%) | | Urological resection | | Partial bladder resection | 11 (52) | | Ureteric resection | 5 (24) | | Partial bladder and ureteric resection | 5 (24) | | Urological reconstructions | | Primary bladder repair only | 10 (48) | | Ureto-uretostomy | 1 (5) | | End-to-end anastomoses | 2 (10) | | Direct implantation | 5 (24) | | Boari flap | 3 (14) |
|
|
|
| Clinical variable | No URR (n = 193) | Operations involving URR (n = 21) | p value | | Age (year)a | 51 ± 12 | 54 ± 12 | 0.23 | | Genderb | 0.6 | | Female | 144 (75) | 14 (67) | | | Male | 49 (25) | 7 (33) | | | Raceb | 0.59 | | Chinese | 146 (75) | 18 (85) | | | Indian | 12 (6) | 1 (5) | | | Malay | 7 (4) | 1 (5) | | | Others | 28 (15) | 1 (5) | | | Primary tumourb | | 0.24 | | Colorectal | 52 (27) | 11 (52) | 0.029 (colorectal vs. other primary tumours) | | Ovarian | 59 (30) | 6 (29) | | | Appendix | 44 (23) | 4 (19) | | | Primary peritoneal | 15 (8) | 0 (0) | | | Others | 13 (7) | 0 (0) | | | Mesothelioma | 10 (5) | 0 (0) | | | Pre-operative stentingb | 44 (23) | 11 (52) | <0.01 | | Previous abdominal surgeryb | 47 (24) | 3 (14) | 0.42 | | Previous pelvic surgeryb | 105 (54) | 16 (76) | 0.065 | | Previous abdominal or pelvic surgeryb | 152 (79) | 19 (90) | 0.26 | | Operative proceduresb | | Subdiaphragmatic stripping | 122 (63) | 6 (29) | <0.01 | | Gastrectomy | 18 (9) | 1 (5) | 0.7 | | Colectomy | 104 (54) | 11 (52) | 1 | | Small bowel resection | 51 (26) | 8 (38) | 0.38 | | Splenectomy | 51 (26) | 3 (14) | 0.3 | | THBSO | 35 (18) | 1 (5) | 0.21 | | Cholecystectomy | 46 (24) | 7 (33) | 0.49 | | PCI scorea | 13 ± 9 | 11 ± 9 | 0.54 | | CC score (median (IQR)) | 0 (0) | 0 (0) | 0.94 | | Duration of procedure (min)a | 490 ± 160 | 570 ± 190 | 0.046 | | Estimated blood loss (mL)a | 1500 ± 1500 | 1300 ± 960 | 0.62 |
|
|
|
|
|
Overall survival following cytoreductive surgery and hyperthermic intraperitoneal chemotherapy, stratified by concomitant urological procedure.
|
| [1] |
B. Sadeghi, C. Arvieux, O. Glehen, A.C. Beaujard, M. Rivoire, J. Baulieux , et al.Peritoneal carcinomatosis from non-gynecologic malignancies: results of the EVOCAPE 1 multicentric prospective study.Cancer, 88(2000), pp. 358-363
doi: 10.1002/(ISSN)1097-0142
|
| [2] |
O. Glehen, F. Kwiatkowski, P.H. Sugarbaker, D. Elias, E.A. Levine, M. DeSimone , et al.Cytoreductive surgery combined with perioperative intraperitoneal chemotherapy for the management of peritoneal carcinomatosis from colorectal cancer: a multi-institutional study.J Clin Oncol, 22(2004), pp. 3284-3292
doi: 10.1200/JCO.2004.10.012
|
| [3] |
V.J. Verwaal, S. Bruin, H. Boot, G. van Slooten, H. van Tinteren . 8-year follow-up of randomized trial: cytoreduction and hyperthermic intraperitoneal chemotherapy versus systemic chemotherapy inpatients with peritoneal carcinomatosis of colorectal cancer.Ann Surg Oncol, 15(2008), pp. 2426-2432
doi: 10.1245/s10434-008-9966-2
pmid: 18521686
|
| [4] |
A. Di Giorgio, E. Naticchioni, D. Biacchi, S. Sibio, F. Accarpio, M. Rocco , et al.Cytoreductive surgery (peritonectomy procedures) combined with hyperthermic intraperitoneal chemotherapy (HIPEC) in the treatment of diffuseperitoneal carcinomatosis from ovarian cancer.Cancer, 113(2008), pp. 315-325
doi: 10.1002/cncr.23553
pmid: 18473354
|
| [5] |
Y. Yonemura, T. Kawamura, E. Bandou, S. Takahashi, T. Sawa, N. Matsuki . Treatment of peritoneal dissemination from gastric cancer by peritonectomy and chemohyperthermic peritoneal perfusion.Br J Surg, 92(2005), pp. 370-375
doi: 10.1002/bjs.4695
pmid: 15739249
|
| [6] |
C. Honore, A. Souadka, D. Goere, F. Dumont, F. Deschamps, D. Elias . HIPEC for peritoneal carcinomatosis: does an associated urologic procedure increase morbidity?Ann Surg Oncol, 19(2012), pp. 104-109
doi: 10.1245/s10434-011-1820-2
pmid: 21638092
|
| [7] |
R.M. Smeenk, A. Bex, V.J. Verwaal, S. Horenblas, F.A. Zoetmulder . Pseudomyxoma peritonei and the urinary tract: involvement and treatment related complications.J Surg Oncol, 93(2006), pp. 20-23
doi: 10.1002/jso.20427
pmid: 16353186
|
| [8] |
K.I. Votanopoulos, R.W. Randle, B. Craven, K.R. Swett, E.A. Levine, P. Shen , et al.Significance of urinary tract involvement in patients treated with cytoreductive surgery (CRS) and hyperthermic intraperitoneal chemotherapy (HIPEC).Ann Surg Oncol, 21(2014), pp. 868-874
doi: 10.1245/s10434-013-3354-2
pmid: 24217789
|
| [9] |
M.S. Leapman, G. Jibara, P. Tabrizian, B. Franssen, M.J. Yang, A. Romanoff , et al.Genitourinary resection at the time of cytoreductive surgery and heated intraperitoneal chemotherapy for peritoneal carcinomatosis is not associated with increased morbidity or worsened oncologic outcomes: a casematched study.Ann Surg Oncol, 21(2014), pp. 1153-1158
doi: 10.1245/s10434-013-3393-8
|
| [10] |
L.S. Krane, A.K. Kader, E.A. Levine . Cytoreductive surgery with hyperthermic intraperitoneal chemotherapy for patients with peritoneal carcinomatosis secondary to urachal adenocarcinoma.J Surg Oncol, 105(2012), pp. 258-260
doi: 10.1002/jso.22081
pmid: 22271499
|
| [11] |
T.D. Lyon, R.B. Turner, T.N. Nikonow, L. Wang, J. Uy, L. Ramalingam , et al.Effect of a concomitant urologic procedure on outcomes following cytoreductive surgery with hyperthermic intraperitoneal chemotherapy.J Surg Oncol, 113(2016), pp. 218-222
doi: 10.1002/jso.24115
pmid: 26775909
|
| [12] |
H.J. Braam, T.R. van Oudheusden, I.H. de Hingh, S.W. Nienhuijs, D. Boerma, M.J. Wiezer , et al.Urological procedures in patients with peritoneal carcinomatosis of colorectal cancer treated with HIPEC: morbidity and survival analysis.Anticancer Res, 35(2015), pp. 295-300
doi: 10.1016/j.ejso.2014.08.046
pmid: 25550563
|
| [13] |
P.H. Sugarbaker . Peritonectomy procedures.Ann Surg, 221(1995), pp. 29-42
doi: 10.1097/00000658-199501000-00004
|
| [14] |
P.H. Sugarbaker, B.M. Ronnett, A. Archer, A.M. Averbach, R. Bland, D. Chang , et al.Pseudomyxoma peritonei syndrome.Adv Surg, 30(1997), pp. 233-280
|
| [15] |
P.H. Sugarbaker . Successful management of microscopic residual disease in large bowel cancer.Cancer Chemother Pharmacol, 43(1999), pp. S15-S25
doi: 10.1007/s002800051093
pmid: 10357554
|
| [16] |
D. Dindo, N. Demartines, P.A. Clavien . Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg, 244(2004), pp. 931-937
|
| [17] |
R Core Team . R: a language and environment for statistical computing.R Foundation for Statistical Computing, Vienna, Austria (2015).
|
| No related articles found! |
|
|
|
|