|
|
|
| Outcomes of combination MRI-targeted and transperineal template biopsy in restaging low-risk prostate cancer for active surveillance |
Kenneth Chena,Kae Jack Taya,Yan Mee Lawb,Hakan Aydinc,Henry Hoa,Christopher Chenga,John Shyi Peng Yuena*( ) )
|
a Department of Urology, Singapore General Hospital, Singapore
b Department of Diagnostic Radiology, Singapore General Hospital, Singapore
c Department of Pathology, Singapore General Hospital, Singapore |
|
|
|
|
Abstract Objective: Active surveillance (AS) offers a strategy to reduce overtreatment and now is a widely accepted treatment option for low-risk prostate cancer. An ideal tool for risk-stratification would detect aggressive cancers and exclude such men from taking up AS in the first place. We evaluate if a combination of transperineal template biopsy with magnetic resonance imaging (MRI)-targeted biopsy identifies significant prostate cancer amongst men initially diagnosed with low-risk prostate cancer. Methods: This prospective, single-blinded study included men with low-risk prostate cancer (D'Amico's Criteria) diagnosed on conventional transrectal ultrasound-guided biopsy. Patients first underwent multiparametric MRI of the prostate ≥6 weeks after initial biopsy. Each suspicious lesion is mapped and assigned a Prostate Imaging Reporting and Data System (PIRADS) score. Template biopsy is first performed with the surgeon blinded to MRI findings followed by MRI-targeted biopsy using a robotic transperineal biopsy platform. Results: The age of the 19 men included is 65.4 ± 4.9 years (mean ± SD). Prostate specific antigen (PSA) at diagnosis and at the time of transperineal biopsy were comparable (7.3 ± 1.7 ng/mL and 7.0 ± 1.8 ng/mL, p = 0.67), so were prostate volumes (34.2 ± 8.9 mL and 32.1 ± 13.4 mL, p = 0.28). MRI-targeted biopsy had a higher percentage of cancer detection per core compared to template biopsy (11.7% vs. 6.5%, p = 0.02), this was more than 3 times superior for Gleason 7 disease (5.9% vs. 1.6%, p < 0.01). Four of 18 (22.2%) patients with MRI lesions had significant disease with MRI-targeted biopsy alone. Three of 19 patients (15.8%) had significant disease with template biopsy alone. In combination, both techniques upclassified five patients (26.3%), all of whom underwent radical prostatectomy. Whole mount histology confirmed tumour location and grade. All six patients with PIRADS 5 lesions had cancer detected (66.6% significant disease). Conclusion: A combination of MRI-targeted and template biopsy may optimally risk-classify “low-risk” patients diagnosed on initial conventional transrectal ultrasonography (TRUS) prostate biopsy.
|
|
Received: 18 August 2016
Published: 23 July 2018
|
|
Corresponding Authors:
Shyi Peng Yuen John
E-mail: john.yuen.s.p@singhealth.com.sg
|
|
|

| T2-Weighted | DWI | DCE | | Echo time/Repetition time (ms) | 82/5700 | 93/7700 | 1.76/4.86 | | Slice thickness (mm) | 3 | 3 | 3 | | Matrix | 384 × 384 | 144 × 160 | 154 × 192 | | Field of view (mm) | 200 | 260 | 260 | | Interslice gap (%) | 10 | 10 | 0 |
|
|
|

|
|
Flowchart of trial protocol. MRI, magnetic resonance imaging; PIRADS, Prostate Imaging Reporting and Data System; PSA, prostate specific antigen; TRUS, transrectal ultrasonography.
|
| Baseline characteristics | TRUS biopsy | rTPB | MRTB | p-Value | | Age (year)a | | 65.4 ± 4.9 | | | PSA at biopsy (ng/mL)a | 7.3 ± 1.7 | 7.0 ± 1.8 | 0.67 | | Interval of last PSA to biopsy (week)b | 4 (1-11) | 8 (4-57) | | | Prostate volume at biopsy (mL)a | 34.2 ± 8.9 | 32.1 ± 13.4 | 0.28 |
|
|
|
| Variables | MRTB | rTPB | p-Value | | Total no. of cores | 239 | 511 | | | No. of positive cores | 28 | 33 | | | No. of Gleason 7 cores | 14 | 8 | | | Percentage of cancer detection per core (%) | 11.7 | 6.5 | 0.02 | | Percentage of Gleason 7 detection per core (%) | 5.9 | 1.6 | <0.01 | | Per patient analysis (mean ± SD) | | No. of biopsy cores | 13.3 ± 5.8 | 26.9 ± 8.2 | <0.05 | | Biopsy intensity (cores/mL) | | 0.87 ± 0.12 | | | No. of positive cores | 1.56 ± 2.79 | 1.74 ± 2.23 | 0.83 | | Max percentage core (%) | 25.6 ± 29.6 | 9.40 ± 9.15 | 0.03 |
|
|
|
|
|
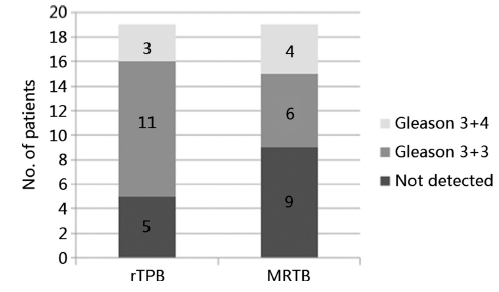
Proportion of upclassification with rTPB and MRTB. MRTB, magnetic resonance imaging-targeted prostate biopsy; rTPB, robotic transperineal template prostate biopsy.
|

|
|
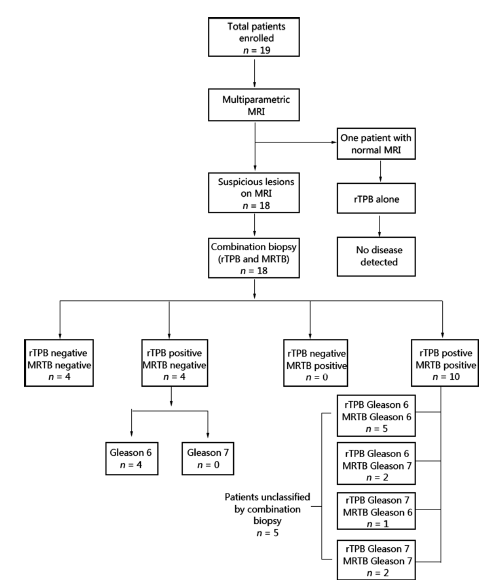
Flow diagram of outcomes of all 19 men. MRI, magnetic resonance imaging; MRTB, MRI-targeted prostate biopsy; rTPB, robotic transperineal template prostate biopsy.
|
| Patient code | Age (year) | PSA at biopsy (ng/mL) | Prostate volume (mL) | MRI highest PIRADS | rTPB | MRTB | | No. positive cores/total cores taken | Gleason score | No. positive cores/total cores taken | Gleason score | | 1 | 75 | 6.2 | 33.3 | 4 | 0/22 | NA | 0/8 | NA | | 2 | 65 | 8.3 | 40.0 | 4 | 1/28 | 6 | 0/10 | NA | | 3a | 61 | 5.6 | 31.0 | 5 | 10/26 | 7 | 2/18 | 7 | | 4 | 71 | 7.0 | 37.0 | 4 | 1/26 | 6 | 0/23 | NA | | 5 | 59 | 9.7 | 17.5 | 5 | 1/18 | 6 | 2/18 | 6 | | 6 | 63 | 7.1 | 22.0 | NA | 0/20 | NA | NA | NA | | 7 | 66 | 8.2 | 37.0 | 4 | 1/27 | 6 | 0/18 | NA | | 8b | 58 | 5.8 | 21.0 | 4 | 2/24 | 7 | 1/12 | 6 | | 9 | 68 | 7.6 | 36.6 | 4 | 2/28 | 6 | 0/8 | NA | | 10c | 68 | 9.9 | 14.0 | 5 | 3/17 | 6 | 12/12 | 7 | | 11c | 68 | 5.8 | 20.0 | 5 | 2/20 | 6 | 3/6 | 7 | | 12 | 69 | 10.0 | 49.0 | 3 | 0/32 | NA | 0/6 | NA | | 13 | 72 | 6.1 | 60.0 | 4 | 3/52 | 6 | 1/19 | 6 | | 14 | 58 | 4.7 | 58.0 | 3 | 0/38 | NA | 0/24 | NA | | 15 | 71 | 7.8 | 28.7 | 5 | 2/23 | 6 | 2/17 | 6 | | 16 | 64 | 4.0 | 32.0 | 3 | 1/25 | 6 | 2/12 | 6 | | 17a | 61 | 7.0 | 26.0 | 5 | 2/22 | 7 | 2/6 | 7 | | 18 | 63 | 8.2 | 31.0 | 3 | 0/28 | NA | 0/10 | NA | | 19 | 63 | 4.7 | 39.0 | 3 | 2/35 | 6 | 1/12 | 6 |
|
|
|
| Parameters of biopsy quality | Combination biopsy | | Gleason 6 (n = 9) | Gleason 7 (n = 5) | | No. of positive cores compared to TRUS Biopsy | Greater
Equal
Less | 5
3
1 | 5
0
0 | | Volume reclassification (Max core percentage) compared to TRUS Biopsy | Yes
No | 5
4 | 5
0 |
|
|
|
| Variables | MRTB | rTPB | p-Value | | Total No. of cores | 102 | 201 | | | No. of positive cores | 12 | 21 | | | Mean maximum core percentage of positive cores (%) | 27.5 | 16.1 | 0.21 | | Percentage of cancer detection per core (%) | 11.8 | 10.4 | 0.71 |
|
|
|
| Patient | TRUS | rTPB | MRTB | RRP | | Location of positive cores | Gleason | Location of positive cores | Gleason | Location of positive cores | Gleason | Location of tumour | Gleason | | 1 | Unknown | 6 | Mid gland AZ | 6 | Not detected | | Not done | | | 2 | Unknown | | Mid gland AZ | 6 | Not detected | | Not done | | | 3 | Right mid gland PZ | 6 | Right mid gland TZ | 6 | Not detected | | Not done | | | 4 | Right mid gland PZ | 6 | Left mid gland PZ | 6 | Right mid gland PZ | 6 | Not done | | | 5 | Right mid gland PZ | 6 | Midline mid gland PZ | 6 | Right mid gland PZ | 6 | Not done | | | 6 | Right mid gland AZ | 6 | Left mid gland AZ | 6 | Left mid gland AZ | 6 | Not done | | | 7 | Right mid gland AZ | 6 | Right mid gland TZ AZ | 6 | Right mid gland AZ | 6 | Not done | | | 8 | Right mid gland PZ | 6 | Left apex to mid gland TZ PZ | 6 | Not detected | | Left apex to mid gland PZ
Right mid gland PZ | 6
6 | | 9 | Left mid gland AZ | 6 | Right apex AZ | 7 | Left apex to mid gland AZ | 6 | Bilateral AZ | 7 | | 10 | Unknown | 6 | Left base to mid gland AZ | 6 | Left base to mid gland AZ | 6 | Not done | | | 11 | Left mid gland AZ | 6 | Right mid gland TZ
Left mid gland AZ | 7 | Left mid gland AZ | 7 | Left AZ | 7 | | 12 | Right mid gland AZ | 6 | Right base to mid gland TZ | 6 | Right base to mid gland TZ | 7 | Bilateral AZ | 7 | | 13 | Unknown | 6 | Midline apex AZ | 6 | Midline apex AZ | 7 | Bilateral apex AZ | 7 | | 14 | Bilateral mid gland PZ | 6 | Right apex to mid gland TZ PZ | 7 | Right apex to mid gland TZ PZ | 7 | Right apex to mid gland PZ | 7 |
|
|
|

|
|
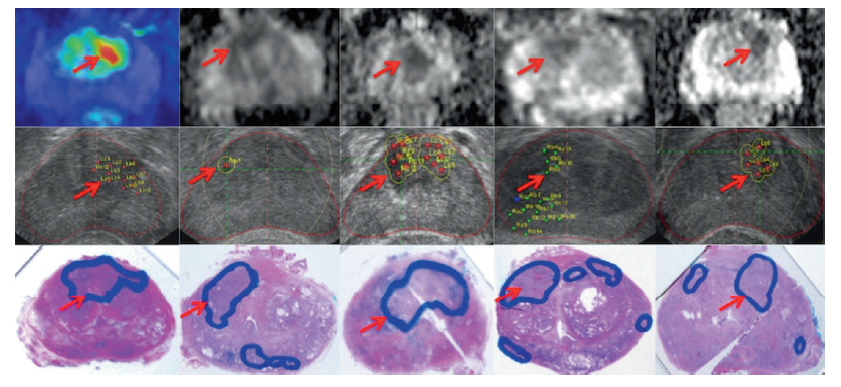
Correlation of multiparametric MRI detected lesions with targeted biopsy plan and whole mount histology. Red arrows point to corresponding lesions and each column represents an individual case. First row shows multiparametric magnetic resonance imaging detected lesions, second row shows the biopsy planning and location of cores, and third row shows the whole mount histology slide.
|
| [1] |
L. Klotz, D. Vesprini, P. Sethukavalan, V. Jethava, L. Zhang, S. Jain , et al.Long-term follow-up of a large active surveillance cohort of patients with prostate cancer.J Clin Oncol, 33(2015), pp. 272-277
doi: 10.1016/j.juro.2015.08.058
pmid: 4827854
|
| [2] |
J.J. Tosoian, M. Mamawala, J.I. Epstein, P. Landis, S. Wolf, B.J. Trock , et al.Intermediate and longer-term outcomes from a prospective active-surveillance program for favorable-risk prostate cancer.J Clin Oncol, 33(2015), pp. 3379-3385
doi: 10.1200/JCO.2015.62.5764
pmid: 4863946
|
| [3] |
T.J. Wilt, M.K. Brawer, K.M. Jones, M.J. Barry, W.J. Aronson, S. Fox , et al.Radical prostatectomy versus observation for localized prostate cancer.N Engl J Med, 367(2012), pp. 203-213
doi: 10.1056/NEJMoa1113162
pmid: 22808955
|
| [4] |
M.A. Dall'Era, P.C. Albertsen, C. Bangma, P.R. Carroll, H.B. Carter, M.R. Cooperberg , et al.Active surveillance for prostate cancer: a systematic review of the literature.Eur Urol, 62(2012), pp. 976-983
doi: 10.1016/j.eururo.2012.05.072
|
| [5] |
A.V. D'Amico, R. Whittington, S.B. Malkowicz, D. Schultz, K. Blank, G.A. Broderick , et al.Biochemical outcome after radical prostatectomy, external beam radiation therapy, or interstitial radiation therapy for clinically localized prostate cancer.JAMA, 280(1998), pp. 969-974
doi: 10.1001/jama.280.11.969
|
| [6] |
Q. Fu, J.W. Moul, L.L. Banez, L. Sun, V. Mouraviev, D. Xie , et al.Association between percentage of tumor involvement and Gleason score upgrading in low-risk prostate cancer.Med Oncol, 29(2012), pp. 3339-3344
doi: 10.1007/s12032-012-0270-4
pmid: 22688447
|
| [7] |
K.J. Tay, M. Mendez, J.W. Moul, T.J. Polascik . Active surveillance for prostate cancer: can we modernize contemporary protocols to improve patient selection and outcomes in the focal therapy era?Curr Opin Urol, 25(2015), pp. 185-190
doi: 10.1097/MOU.0000000000000168
|
| [8] |
B. Turkbey, H. Mani, V. Shah, A.R. Rastinehad, M. Bernardo, T. Pohida , et al.Multiparametric 3T prostate magnetic resonance imaging to detect cancer: histopathological correlation using prostatectomy specimens processed in customized magnetic resonance imaging based molds.J Urol, 186(2011), pp. 1818-1824
doi: 10.1016/j.juro.2011.07.013
|
| [9] |
J.D. Le, N. Tan, E. Shkolyar, D.Y. Lu, L. Kwan, L.S. Marks , et al.Multifocality and prostate cancer detection by multiparametric magnetic resonance imaging: correlation with whole-mount histopathology.Eur Urol, 67(2015), pp. 569-576
doi: 10.1016/j.eururo.2014.08.079
pmid: 25257029
|
| [10] |
C.M. Moore, V. Kasivisvanathan, S. Eggener, M. Emberton, J.J. Futterer, I.S. Gill , et al.Standards of reporting for MRI-targeted biopsy studies (START) of the prostate: recommendations from an International Working Group.Eur Urol, 64(2013), pp. 544-552
doi: 10.1016/j.eururo.2013.03.030
pmid: 23537686
|
| [11] |
H. Ho, J.S. Yuen, P. Mohan, E.W. Lim, C.W. Cheng . Robotic transperineal prostate biopsy: pilot clinical study.Urology, 78(2011), pp. 1203-1208
doi: 10.1016/j.urology.2011.07.1389
pmid: 21940041
|
| [12] |
H.S. Ho, P. Mohan, E.D. Lim, D.L. Li, J.S. Yuen, W.S. Ng , et al.Robotic ultrasound-guided prostate intervention device: system description and results from phantom studies.Int J Med Robot, 5(2009), pp. 51-58
doi: 10.1002/rcs.232
pmid: 19145573
|
| [13] |
M. Rothke, D. Blondin, H.P. Schlemmer, T. Franiel . PI-RADS classification: structured reporting for MRI of the prostate.Rofo, 185(2013), pp. 253-261
|
|
[Article in German]
|
| [14] |
J.O. Barentsz, J. Richenberg, R. Clements, P. Choyke, S. Verma, G. Villeirs , et al.ESUR prostate MR guidelines 2012. Eur Radiol, 22(2012), pp. 746-757
doi: 10.1007/s00330-011-2377-y
pmid: 3297750
|
| [15] |
P. Mufarrij, A. Sankin, G. Godoy, H. Lepor . Pathologic outcomes of candidates for active surveillance undergoing radical prostatectomy.Urology, 76(2010), pp. 689-692
doi: 10.1016/S0022-5347(09)61707-9
|
| [16] |
E.C. Serefoglu, S. Altinova, N.S. Ugras, E. Akincioglu, E. Asil, M.D. Balbay . How reliable is 12-core prostate biopsy procedure in the detection of prostate cancer?Can Urol Assoc J, 7(2013), pp. E293-E298
doi: 10.1016/S1569-9056(10)60075-9
pmid: 3668408
|
| [17] |
F. Rabbani, N. Stroumbakis, B.R. Kava, M.S. Cookson, W.R. Fair . Incidence and clinical significance of false-negative sextant prostate biopsies.J Urol, 159(1998), pp. 1247-1250
doi: 10.1097/00005392-199804000-00047
pmid: 9507846
|
| [18] |
P. Pepe, A. Garufi, G. Priolo, M. Pennisi . Transperineal versus transrectal MRI/TRUS fusion targeted biopsy: detection rate of clinically significant prostate cancer.Clin Genitourin Cancer, 15(2017), pp. e33-e36
doi: 10.1016/j.clgc.2016.07.007
pmid: 27530436
|
| [19] |
T.H. Kuru, K. Wadhwa, R.T. Chang, L.M. Echeverria, M. Roethke, A. Polson , et al.Definitions of terms, processes and a minimum dataset for transperineal prostate biopsies: a standardization approach of the Ginsburg Study Group for Enhanced Prostate Diagnostics.BJU Int, 112(2013), pp. 568-577
doi: 10.1111/bju.12132
pmid: 23773772
|
| [20] |
A. Sivaraman, R. Sanchez-Salas, E. Barret, Y. Ahallal, F. Rozet, M. Galiano , et al.Transperineal template-guided mapping biopsy of the prostate.Int J Urol, 22(2015), pp. 146-151
doi: 10.1111/iju.12660
pmid: 25421717
|
| [21] |
M. Valerio, C. Anele, S.C. Charman, J. van der Meulen, A. Freeman, C. Jameson , et al.Transperineal template prostate-mapping biopsies: an evaluation of different protocols in the detection of clinically significant prostate cancer.BJU Int, 118(2016), pp. 384-390
doi: 10.1111/bju.13306
|
| [22] |
A.P. Kirkham, M. Emberton, C. Allen . How good is MRI at detecting and characterising cancer within the prostate?Eur Urol, 50(2006), pp. 1163-1174
doi: 10.1016/j.eururo.2006.06.025
pmid: 16842903
|
| [23] |
A. Villers, L. Lemaitre, J. Haffner, P. Puech . Current status of MRI for the diagnosis, staging and prognosis of prostate cancer: implications for focal therapy and active surveillance.Curr Opin Urol, 19(2009), pp. 274-282
doi: 10.1097/MOU.0b013e328329a2ed
pmid: 19325494
|
| [24] |
S.S. Dianat, H.B. Carter, K.J. Macura . Magnetic resonance-guided prostate biopsy.Magn Reson Imaging Clin N Am, 23(2015), pp. 621-631
doi: 10.1016/j.mric.2015.05.005
pmid: 26499279
|
| [25] |
J.S. Wysock, A.B. Rosenkrantz, W.C. Huang, M.D. Stifelman, H. Lepor, F.M. Deng , et al.A prospective, blinded comparison of magnetic resonance (MR) imaging-ultrasound fusion and visual estimation in the performance of MR-targeted prostate biopsy: the PROFUS trial.Eur Urol, 66(2014), pp. 343-351
doi: 10.1016/j.eururo.2013.10.048
|
| [26] |
M.M. Siddiqui, S. Rais-Bahrami, H. Truong, L. Stamatakis, S. Vourganti, J. Nix , et al.Magnetic resonance imaging/ultrasound-fusion biopsy significantly upgrades prostate cancer versus systematic 12-core transrectal ultrasound biopsy.Eur Urol, 64(2013), pp. 713-719
doi: 10.1016/j.eururo.2013.05.059
pmid: 2378735720
|
| [27] |
G.A. Sonn, E. Chang, S. Natarajan, D.J. Margolis, M. Macairan, P. Lieu , et al.Value of targeted prostate biopsy using magnetic resonance-ultrasound fusion in men with prior negative biopsy and elevated prostate-specific antigen.Eur Urol, 65(2014), pp. 809-815
doi: 10.1016/j.eururo.2013.03.025
pmid: 3858524
|
| [28] |
Y. Cerantola, E. Haberer, J. Torres, M. Alameldin, S. Aronson, M. Levental , et al.Accuracy of cognitive MRI-targeted biopsy in hitting prostate cancer-positive regions of interest.World J Urol, 34(2016), pp. 75-82
doi: 10.1007/s00345-015-1588-2
pmid: 25981403
|
| [29] |
P. Pepe, A. Garufi, G. Priolo, M. Pennisi . Can MRI/TRUS fusion targeted biopsy replace saturation prostate biopsy in the re-evaluation of men in active surveillance?World J Urol, 34(2016), pp. 1249-1253
doi: 10.1007/s00345-015-1749-3
pmid: 26699628
|
| [30] |
P. Recabal, M. Assel, D.D. Sjoberg, D. Lee, V.P. Laudone, K. Touijer . The efficacy of multiparametric magnetic resonance imaging and magnetic resonance imaging targeted biopsy in risk classification for patients with prostate cancer on active surveillance.J Urol, 196(2016), pp. 374-381
doi: 10.1016/j.juro.2016.02.084
pmid: 26920465
|
| [1] |
Edwin Jonathan Aslim,Yan Mee Law,Puay Hoon Tan,John Carson Allen Jr,Lionel Tim-Ee Cheng,Viswanath Anand Chidambaram,Li Yan Khor,Benjamin Yongcheng Tan,Ernest Wencong Eu,Christopher Wai Sam Cheng,John Shyi Peng Yuen,Henry Sun Sien Ho,Lui Shiong Lee. Multiparametric MRI reporting using Prostate Imaging Reporting and Data System version 2.0 (PI-RADSv2) retains clinical efficacy in a predominantly post-biopsy patient population[J]. Asian Journal of Urology, 2019, 6(3): 256-263. |
| [2] |
Laurence Klotz. Contemporary approach to active surveillance for favorable risk prostate cancer[J]. Asian Journal of Urology, 2019, 6(2): 146-152. |
| [3] |
Olivier Rouviere , Paul Cezar Moldovan. The current role of prostate multiparametric magnetic resonance imaging[J]. Asian Journal of Urology, 2019, 6(2): 137-145. |
| [4] |
Jean-Luc Descotes. Diagnosis of prostate cancer[J]. Asian Journal of Urology, 2019, 6(2): 129-136. |
| [5] |
Geoffrey Gaunay, Vinay Patel, Paras Shah, Daniel Moreira, Simon J. Hall, Manish A. Vira, Michael Schwartz, Jessica Kreshover, Eran Ben-Levi, Robert Villani, Ardeshir Rastinehad, Lee Richstone. Role of multi-parametric MRI of the prostate for screening and staging: Experience with over 1500 cases[J]. Asian Journal of Urology, 2017, 4(1): 68-74. |
| [6] |
Geoffrey S. Gaunay, Vinay Patel, Paras Shah, Daniel Moreira, Ardeshir R. Rastinehad, Eran Ben-Levi, Robert Villani, Manish A. Vira. Multi-parametric MRI of the prostate: Factors predicting extracapsular extension at the time of radical prostatectomy[J]. Asian Journal of Urology, 2017, 4(1): 31-36. |
|
|
|
|