|
|
2016年, 第3卷, 第3期 刊出日期:2016-07-01
|
上一期
下一期 |
|
|
|
|
|
Recent advances in oncological endourology
Allen W. Chiu
Asian Journal of Urology, 2016, 3(3): 113-114.
doi:10.1016/j.ajur.2016.05.005
 摘要
摘要
(
395 )
 PDF
PDF (374KB)
(
321
)
It has been almost four decades since we urologists intensively started to embrace the techniques of endoscopic surgery, and applied it into our daily clinical practice. Endourology has actually revolutionized the practice pattern of not only academic but also practicing urologists worldwide. Since early 1990, the advent of laparoscopic surgery and later robotic assisted surgery truly witnessed the progress of the minimally invasive therapy in Urology. I am honored to have this opportunity to invite world renowned scholars to contribute into this special issue entitled “Recent Advances in Oncological Endourology” in Asian Journal of Urology. I would like to express my gratitude for their efforts. The concept of minimally invasive surgical technique has gathered great attention from physicians as well as our patients. Without question, the driving force is multifactorial, which includes tremendous progress in modern mechanical and intelligent technology, the acceptance of minimally invasive concept by patients and the broadcasting effects by the media.
参考文献 |
相关文章 |
计量指标
|
|
|
Laparoscopic nephroureterectomy for upper tract urothelial carcinoma e Update
Victor C. Lin, Chung-hsien Chen, Allen W. Chiu,
Asian Journal of Urology, 2016, 3(3): 115-119.
doi:10.1016/j.ajur.2016.05.003
摘要
(
608 )
PDF (401KB)
(
457
)
Upper urinary tract urothelial carcinomas (UTUCs) are uncommon and account for only 5%e10% of urothelial carcinomas. Pyelocaliceal tumors are about twice as common as ureteral tumors. Sixty percent of UTUCs are invasive at diagnosis. Radical nephroureterectomy, including the excision of the distal ureter and bladder cuff is standard of care for treatment of localized UTUCs, because of the high potential for recurrence, multifocality, and progression. Since first laparoscopic nephroureterectomy (LNU) was introduced by Clayman et al. in 1991 and improvement of laparoscopic technique and equipment, LNU has been reported to be equivalent to conventional open method. We reviewed the current literature of patients with UTUCs treated by LNU focusing on technical aspects, peri-operative and oncological outcomes. Laparoscopic radical nephroureterectomy offers the advantages of minimally invasive surgery without deteriorating the oncological outcome for treatment of UTUCs. Indications tend to increase as operator skills increase. Indications for laparoscopic or open nephroureterectomy are in principle the same. The basic requirement for laparoscopic surgery in UTUCs is to achieve benefits of minimal invasive surgery and maintain oncologic principles.
参考文献 |
相关文章 |
计量指标
|
|
|
Techniques to resect the distal ureter in robotic/laparoscopic nephroureterectomy
Weil R. Lai, Benjamin R. Lee
Asian Journal of Urology, 2016, 3(3): 120-125.
doi:10.1016/j.ajur.2016.04.001
摘要
(
516 )
PDF (672KB)
(
561
)
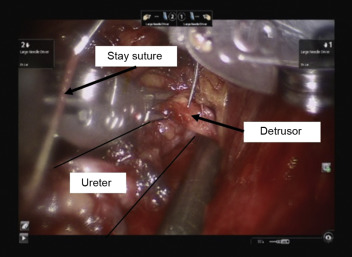
Treatment of clinically-organ confined high grade urothelial carcinoma of the upper tract has historically comprised open nephroureterectomy, with the distal ureter and bladder cuff mobilized through a separate open pelvic incision. To decrease morbidity, urologists have increasingly adopted laparoscopy and robotics in performing nephroureterectomy. In many published series of laparoscopic nephroureterectomy, the distal ureter and bladder cuff are detached from the bladder endoscopically by a variation of the “pluck” technique, with the resulting bladder defect left to heal by prolonged indwelling urethral catheter drainage. While the distal ureter and bladder cuff can be excised laparoscopically, it does require advanced laparoscopic skills. With the wrist articulation and stereoscopic vision in robotic surgery, robotic nephroureterectomy (RNU) and bladder cuff excision can be performed in antegrade fashion to mimic the open technique together with the ability to intracorporeally close the bladder defect in a watertight, mucosa to mucosa fashion after excising the bladder cuff. In this review, we discuss the published minimally invasive techniques in resecting the distal ureter and bladder cuff during laparoscopic and RNU.
参考文献 |
相关文章 |
计量指标
|
|
|
Narrow band imaging for bladder cancer
Thomas Y. Hsueh, Allen W. Chiu
Asian Journal of Urology, 2016, 3(3): 126-129.
doi:10.1016/j.ajur.2016.05.001
摘要
(
324 )
PDF (393KB)
(
194
)
Narrow band imaging (NBI) is a newly developed technology aiming to provide additional endoscopic information for patients with bladder cancer. This review focuses on the diagnostic accuracy and treatment outcome using NBI cystoscopy for the treatment of nonmuscle invasive bladder cancer. Current results showed improved sensitivity of NBI cystoscopy compared to conventional white light cystoscopy, although lower specificity and increased false-positive results were reported using NBI cystoscopy. The treatment outcome using NBI technology in transurethral resection of bladder tumor had a positive impact while decreased number of residual tumors and tumor recurrence at follow-up were reported. In the future, the application of NBI technology might refine the treatment and follow-up protocol in patients with non-muscle invasive bladder cancer. However, this large scale prospective studies are required to confirm the real cost-effectiveness of this new technology.
参考文献 |
相关文章 |
计量指标
|
|
|

Thulium laser treatment for bladder cancer
Wei Wang, Haitao Liu, Shujie Xia
Asian Journal of Urology, 2016, 3(3): 130-133.
doi:10.1016/j.ajur.2016.05.002
摘要
(
412 )
PDF (394KB)
(
529
)
Recent innovations in thulium laser techniques have allowed application in the treatment of bladder cancer. Laser en bloc resection of bladder cancer is a transurethral procedure that may offer an alternative to the conventional transurethral resection procedure. We conducted a review of basic thulium laser physics and laser en bloc resection procedures and summarized the current clinical literature with a focus on complications and outcomes. Literature evidence suggests that thulium laser techniques including smooth incision, tissue vaporization, and en bloc resection represent feasible, safe, and effective procedures in the treatment of bladder cancer. Moreover, these techniques allow improved specimen orientation and accurate determination of invasion depth, facilitating correct diagnosis, restaging, and reevaluation of the need for a second resection. Nonetheless, large-scale multicentre studies with longer follow-up are warranted for a robust assessment. The present review is meant as a quick reference for urologists.
参考文献 |
相关文章 |
计量指标
|
|
|
Percutaneous resection of upper tract urothelial cell carcinoma: When, how, and is it safe?
Willem E. Strijbos, Bart van der Heij
Asian Journal of Urology, 2016, 3(3): 134-141.
doi:10.1016/j.ajur.2016.04.003
摘要
(
407 )
PDF (2434KB)
(
564
)
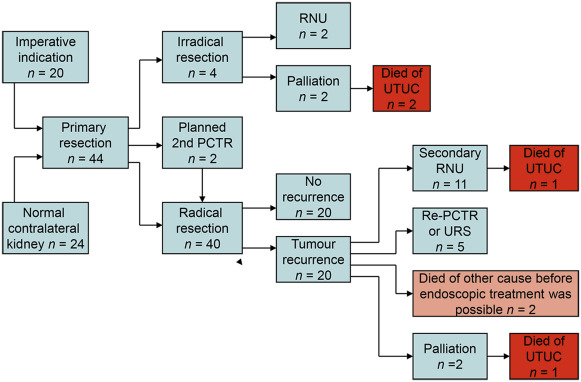
Introduction: In the management of upper tract urothelial cell carcinoma (UTUC) endoscopic, nephron sparing procedures like ureterorenoscopy (URS) or percutaneous tumour resection (PCTR) still play a very limited role. This could lead to possible unnecessary radical nephroureterectomies (RNU), still being the gold standard treatment. The risk of chronic kidney disease (CKD) later in life is important. In this study we present the results of 24-year experience with PCTR in a single institution.
Methods: We identified 44 patients who underwent PCTR between 1992 and 2015. Radical resection was achieved in 40 patients who were included in this study. Demographic and clinical data, including tumour recurrence, progression to RNU, tumour grade and overall survival (OS) were retrospectively acquired. An outcome analysis was conducted. Results: Median age at diagnosis was 68 years (range 42e94 years). Low grade tumours were found in 37 patients (92.5%) and high grade tumours in three patients (7.5%). Median followup was 53 months during which 20 patients developed upper tract recurrences (50.0%). The longest time to recurrence was 97 months. At follow-up 11 patients (27.5%) underwent an RNU and two patients died from UTUC. RNU could be avoided in 29 patients (72.5%). In this study we found that multifocality is a significant risk factor for recurrence, but not for stage progression to RNU.
Conclusion: PCTR is a surgically and oncologically safe procedure. Renal preservation in patients with UTUC who are eligible for percutaneous resection can be achieved in the majority of patients. Selection criteria for PCTR should be further refined, leading to a wider application of PCTR in the future. Follow-up needs invasive procedures and should be long term.
参考文献 |
相关文章 |
计量指标
|
|
|

Stents for malignant ureteral obstruction
Kristina Pavlovic, Dirk Lange, Ben H. Chew
Asian Journal of Urology, 2016, 3(3): 142-149.
doi:10.1016/j.ajur.2016.04.002
摘要
(
463 )
PDF (956KB)
(
205
)
Malignant ureteral obstruction can result in renal dysfunction or urosepsis and can limit the physician's ability to treat the underlying cancer. There are multiple methods to deal with ureteral obstruction including regular polymeric double J stents (DJS), tandem DJS, nephrostomy tubes, and then more specialized products such as solid metal stents (e.g., Resonance Stent, Cook Medical) and polyurethane stents reinforced with nickel-titanium (e.g., UVENTA stents, TaeWoong Medical). In patients who require long-term stenting, a nephrostomy tube could be transformed subcutaneously into an extra-anatomic stent that is then inserted into the bladder subcutaneously. We outline the most recent developments published since 2012 and report on identifiable risk factors that predict for failure of urinary drainage. These failures are typically a sign of cancer progression and the natural history of the disease rather than the individual type of drainage device. Factors that were identified to predict drainage failure included low serum albumin, bilateral hydronephrosis, elevated C-reactive protein, and the presence of pleural effusion. Head-to-head studies show that metal stents are superior to polymeric DJS in terms of maintaining patency. Discussions with the patient should take into consideration the frequency that exchanges will be needed, the need for externalized hardware (with nephrostomy tubes), or severe urinary symptoms in the case of internal DJS. This review will highlight the current state of diversions in the setting of malignant ureteral obstruction.
参考文献 |
相关文章 |
计量指标
|
|
|

Current status of laparoscopic and robotassisted nerve-sparing radical cystectomy in male patients
Jian Huang, Xinxiang Fan, Wen Dong
Asian Journal of Urology, 2016, 3(3): 150-155.
doi:10.1016/j.ajur.2016.04.004
摘要
(
412 )
PDF (403KB)
(
757
)
During radical cystectomy (RC), the neurovascular bundles are easily removed or damaged, leading to varying rates of incontinence and erectile dysfunction. The nervesparing technique was developed to preserve urinary and erectile function. The adoption of laparoscopic and robot-assisted technology has improved visualization and dexterity of pelvic surgeries, thus facilitate the nerve-sparing technique. Although nerve-sparing RC is technically similar with nerve-sparing radical prostatectomy, there are still some anatomical differences. There are mainly three different types of nerve-sparing techniques. Pelvic lymph node dissection (PLND) is another important factor to influence erectile function and urinary continence. Nerve-sparing laparoscopic radical cystectomy (LRC) and robot-assisted radical cystectomy (RARC) may be an optimal treatment choice in well-selected younger patients with lowvolume, organ-confined disease. We should attempt to do, whenever possible, a nerve-sparing cystectomy at least on oneside. However, due to the need of a well-refined surgical technique, nerve-sparing LRC and RARC is now being performed only by experienced urological surgeons.
参考文献 |
相关文章 |
计量指标
|
|
|
Robot-assisted laparoscopic radical cystectomy with complete intracorporeal urinary diversion
Jason M. Sandberg, Ashok K. Hemal
Asian Journal of Urology, 2016, 3(3): 156-166.
doi:10.1016/j.ajur.2016.05.004
摘要
(
448 )
PDF (446KB)
(
402
)
Robot-assisted radical cystectomy with intracorporeal urinary diversion (RARCICUD) has only recently been explored as a viable surgical option for patients with muscle-invasive bladder cancer seeking satisfactory oncologic control while benefiting from minimally invasive surgical techniques. Inspired by earlier open and laparoscopic work, initial descriptions of RARC-ICUD were published in 2003, and have since been followed by multiple larger case series which have suggested promising outcomes for our patients. However, the rate of adoption has remained relatively slow when compared to other robotassisted procedures such as the radical prostatectomy, likely owing to longer operative times, operative complexity, costs, and uncertainty regarding oncologic efficacy. The operative technique for RARC-ICUD has evolved over the past decade and several high-volume centers have shared tips to improve efficiency and make the operation possible for a growing number of urologists. Though there are still questions regarding economic costs, effectiveness, and generalizability of outcomes reported in published data, a growing dataset has brought us ever closer to the answers. Here, we present our current operative technique for RARC-ICUD and discuss the state of the literature so that the urologist may hold an informed discussion with his or her patients.
参考文献 |
相关文章 |
计量指标
|
|





 当期目录
当期目录
