|
|
2015年, 第2卷, 第4期 刊出日期:2015-10-01
|
上一期
下一期 |
|
|
|
|
|
Contemporary outcomes in the detection of prostate cancer using transrectal ultrasound-guided 12-core biopsy in Singaporean men with elevated prostate specific antigen and/or abnormal digital rectal examination
Alvin Lee, Sing Joo Chia
Asian Journal of Urology, 2015, 2(4): 187-193.
doi:10.1016/j.ajur.2015.08.003
 摘要
摘要
(
497 )
 PDF
PDF (416KB)
(
304
)
Objective: Despite being the third commonest cancer in Singaporean men, there is a dearth of basic data on the detection rate of prostate cancer and post-procedure complication rates locally using systematic 12-core biopsy. Our objective is to evaluate prostate cancer detection rates using 12-core prostate biopsy based on serum prostate specific antigen (PSA) levels and digital rectal examination (DRE) findings in Singaporean men presenting to a single tertiary centre. The secondary objective is to evaluate the complication rates of transrectal prostate biopsies.Methods: We retrospectively examined 804 men who underwent first transrectal-ultrasound (TRUS) guided 12-core prostate biopsies from January 2012 to April 2014. Prostate biopsies were performed on men presenting to a tertiary institution when their PSA levels were≥4.0 ng/mL and/or when they had suspicious DRE findings.Results: Overall prostate cancer detection rate was 35.1%. Regardless of DRE findings, patients were divided into four subgroups based on their serum PSA levels: 0-3.99 ng/mL, 4.00 -9.99 ng/mL, 10.00-19.99 ng/mL and≥20.00 ng/mL and their detection rates were 9.5%, 20.9%, 38.4% and 72.3%, respectively. The detection rate of cancer based on suspicious DRE findings alone was 59.2% compared to 36.5% based on serum PSA cut-off of 4.0 ng/mL alone. The post-biopsy admission rate for sepsis was 1.5%.
参考文献 |
相关文章 |
计量指标
|
|
|

Ureteral stent technology: Drug-eluting stents and stent coatings
Luo Yang, Samantha Whiteside, Peter A. Cadieux, John D. Denstedt
Asian Journal of Urology, 2015, 2(4): 194-201.
doi:10.1016/j.ajur.2015.08.006
摘要
(
402 )
PDF (422KB)
(
312
)
Ureteral stents are commonly used following urological procedures to maintain ureteral patency. However, alongside the benefits of the device, indwelling stents frequently cause significant patient discomfort (pain, urgency, frequency) and can become encrusted and infected. The importance of these sequelae is that they are not only bothersome to the patient but can lead to significant morbidity, urinary retention, ureteral damage, recurrent infections, pyelonephritis and sepsis. When these problems occur, stent removal or replacement alongside antibiotic, analgesic and/or other symptom-modifying therapies are essential to successfully treat the patient. In an attempt to prevent such morbidity, numerous approaches have been investigated over the past several decades to modify the stent itself, thereby affecting changes locally within the urinary tract without significant systemic therapy. These strategies include changes to device design, polymeric composition, drug-elution and surface coatings. Of these, drug-elution and surface coatings are the most studied and display the most promise for advancing ureteral stent use and efficacy. This article reviews these two strategies in detail to determine their clinical potential and guide future research in the area.
参考文献 |
相关文章 |
计量指标
|
|
|
Diagnosis and management of ureteral complications following renal transplantation
Brian D. Duty, John M. Barry
Asian Journal of Urology, 2015, 2(4): 202-207.
doi:10.1016/j.ajur.2015.08.002
摘要
(
460 )
PDF (1695KB)
(
450
)
When compared with maintenance dialysis, renal transplantation affords patients with end-stage renal disease better long-term survival and a better quality of life. Approximately 9% of patients will develop a major urologic complication following kidney transplantation. Ureteral complications are most common and include obstruction (intrinsic and extrinsic), urine leak and vesicoureteral reflux. Ureterovesical anastomotic strictures result from technical error or ureteral ischemia. Balloon dilation or endoureterotomy may be considered for short, low-grade strictures, but open reconstruction is associated with higher success rates. Urine leak usually occurs in the early postoperative period. Nearly 60% of patients can be successfully managed with a pelvic drain and urinary decompression (nephrostomy tube, ureteral stent, and indwelling bladder catheter). Proximal, large-volume, or leaks that persist despite urinary diversion, require open repair. Vesicoureteral reflux is common following transplantation. Patients with recurrent pyelonephritis despite antimicrobial prophylaxis require surgical treatment. Deflux injection may be considered in recipients with low-grade disease. Grade IV and V reflux are best managed with open reconstruction.
参考文献 |
相关文章 |
计量指标
|
|
|
Percutaneous nephrolithotomy in octogenarians and beyond: How old is too old?
Bradley Morganstern, Riccardo Galli, Piruz Motamedinia, David Leavitt, Mohamed Keheila, Eric Ghiraldi, David Hoenig, Arthur Smith, Zeph Okeke
Asian Journal of Urology, 2015, 2(4): 208-213.
doi:10.1016/j.ajur.2015.08.005
摘要
(
382 )
PDF (403KB)
(
390
)
Objective: To specifically report perioperative characteristics and outcomes in patients 80 years and older undergoing percutaneous nephrolithotomy (PCNL). PCNL has been established as feasible in the elderly; however, to our knowledge no one has specifically reported feasibility in patients 80 years and older. Methods: We retrospectively reviewed perioperative data of octogenarians who underwent PCNL at a high stone volume single institution, and matched them to patients <65 years of age by stone burden and sex. Patient demographics, perioperative outcomes and postoperative complications were compared. Results: Thirty-three octogenarians (mean age 83.6 years) with 36 renal units were matched to 67 controls (mean age 48.6 years) with 72 renal units. Octogenarians had a higher mean American Society of Anesthesiologists (ASA) score, more comorbidities, and worse renal function. There were no differences in operative characteristics, length of hospital stay or stone free rates. Of the patients with preoperative urinary decompression (ureteral stent or nephrostomy tube) prior to PCNL, the elderly were more likely to have a history of urosepsis. Octogenarians did not experience more minor Clavien (I-II) or major Clavien (IIIa-IVb) complications. Conclusion: Octogenarians who undergo PCNL were more likely to have cardiovascular comorbidities and a prior history of sepsis. Despite these risk factors, in appropriately selected patients PCNL can be safely and successfully performed in octogenarians without increased perioperative complications relative to a younger cohort.
参考文献 |
相关文章 |
计量指标
|
|
|
Three-dimensional printing technique assisted cognitive fusion in targeted prostate biopsy
Yan Wang, Xu Gao, Qingsong Yang, Haifeng Wang, Ting Shi, Yifan Chang, Chuanliang Xu, Yinghao Sun
Asian Journal of Urology, 2015, 2(4): 214-219.
doi:10.1016/j.ajur.2015.09.002
摘要
(
329 )
PDF (1819KB)
(
334
)
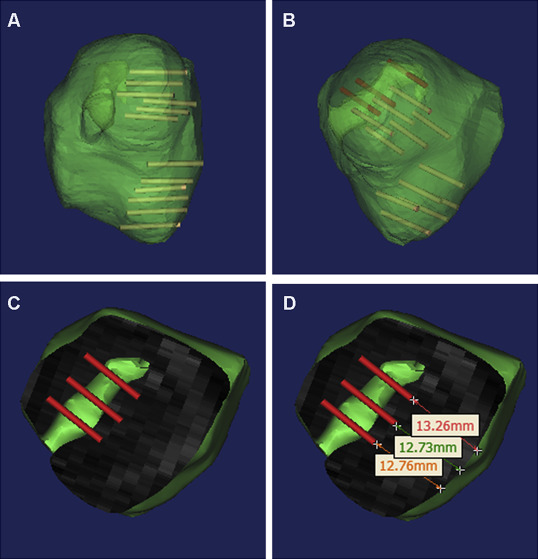
Objective: To explore the effect of 3-dimensional (3D) printing-assisted cognitive fusion on improvement of the positive rate in prostate biopsy. Methods: From August to December 2014, 16 patients with suspected prostatic lesions detected by multiparametric magnetic resonance imaging (MRI) were included. Targeted prostate biopsy was performed with the use of prostate 3D reconstruction modeling, computersimulated biopsy, 3D printing, and cognitive fusion biopsy. All patients had received 3.0 T multiparametric MRI before biopsy. The DICOM MRI files were imported to medical imaging processing software for 3D reconstruction modeling to generate a printable .stl file for 3D printing with use of transparent resin as raw material. We further performed a targeted 2- to 3-core biopsy at suspected lesions spotted on MRI. Results: For the 16 patients in the present study, 3D modeling with cognitive fusion-based targeted biopsy was successfully performed. For a single patient, 1-2 lesions (average: 1.1 lesions) were discovered, followed by 2-6 cores (average: 2.4 cores) added as targeted biopsy. Systematic biopsies accounted for 192 cores in total, with a positive rate of 22.4%; targeted biopsies accounted for 39 cores in total, with a positive rate of 46.2%. Among these cases, 10 patients (62.5%) were diagnosed with prostate adenocarcinoma, in which seven were discovered by both systematic and targeted biopsy, one was diagnosed by systematic biopsy only, and two were diagnosed by targeted biopsy only. For systematic biopsy, Gleason score ranged from 6 to 8 (average: 7), while that for targeted biopsy ranged from 6 to 9 (average: 7.67). Among the seven patients that were diagnosed by both systematic and targeted biopsy, three (42.8%) were reported with a higher Gleason score in targeted therapy than in systematic biopsy.
参考文献 |
相关文章 |
计量指标
|
|
|
Does the presence of a percutaneous renal access influence fluoroscopy time during percutaneous nephrolithotomy?
Yasser A. Noureldin, Mohamed A. Elkoushy, Sero Andonian
Asian Journal of Urology, 2015, 2(4): 220-223.
doi:10.1016/j.ajur.2015.08.001
摘要
(
479 )
PDF (389KB)
(
300
)
Objective: The aim of this study was to assess whether the presence of a preformed percutaneous renal access (PCA) had any effects on fluoroscopy time (FT) during percutaneous nephrolithotomy (PCNL). Methods: After ethics approval was obtained, medical records of all patients who underwent PCNL between 2009 and 2013 at a tertiary stone referral centre were retrospectively reviewed. Patients with and without pre-formed PCA undergoing PCNL were compared. Patients who underwent second-look PCNL and those who had their access inserted by interventional radiology constituted the group with pre-formed PCA. Results: A total of 185 PCNLs were reviewed. The mean patient age was 55.2± 1.0 years with mean body mass index (BMI) of 27.8± 0.5 kg/m2 and male gender of 63.8%. The mean stone size was 618.4± 47.0 mm2 with mean Guy's grade of 2.3± 0.7 and mean S.T.O.N.E. score of 7.6± 0.1. The mean operative time was 98.7± 2.6 min with mean FT of 113.4± 4.5 s. The overall stone-free rate was 71.9% with complication rate of 16.2%. When compared with PCNLs without pre-formed PCA, PCNLs with pre-formed PCA were associated with significantly shorter FT (120.6± 5.1 vs. 77.5± 6.7 s; p < 0.001) and significantly lower estimated blood loss (EBL) (p = 0.01). On multivariate analysis, PCNLs with pre-formed PCA were associated with significantly shorter FT (B. coefficient =±43.2 (95%CI:±66.4 to±20); p < 0.001) and lower EBL (p = 0.02).
参考文献 |
相关文章 |
计量指标
|
|
|
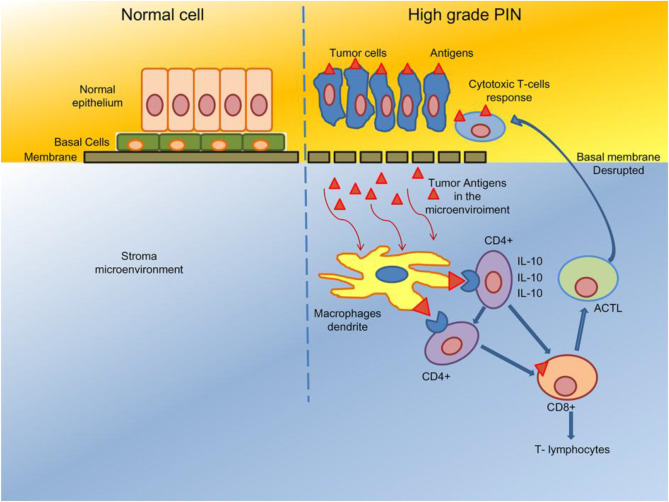
Prostate chronic inflammation type IV and prostate cancer risk in patients undergoing first biopsy set: Results of a large cohort study
Antonio Benito Porcaro, Giovanni Novella, Matteo Balzarro, Guido Martignoni, Matteo Brunelli, Giovanni Cacciamani, Maria A. Cerruto, Walter Artibani
Asian Journal of Urology, 2015, 2(4): 224-232.
doi:10.1016/j.ajur.2015.08.007
摘要
(
537 )
PDF (3242KB)
(
696
)
Objective: In prostate specimens, chronic inflammatory infiltrate (CII) type IV has been detected, but its association with prostate cancer (PCa) is controversial. The aim of the present study is to investigate on associations of CII with PCa detection in patients undergoing prostate first biopsy set. Methods: Ultrasound transrectal-guided biopsies by the transperineal approach were retrospectively evaluated in 441 consecutive patients. The study excluded patients who were in active surveillance, prostate specific antigen (PSA)≥30 ng/mL, re-biopsies, incidental PCa after transurethral resection of the prostate (TURP), less than 14 cores or metastatic. Analysis of population and subpopulations (with or without PCa) was performed by statistical methods which included ManneWhitney (U test), Kruskal-Wallis test, Chi-squared statistic, logistic regression. Multivariate logistic regression models predicting mean probability of PCa detection were established. Results: PCa detection rate was 46.03%. Age, PSA, prostate volume (PV), prostate intraepithelial neoplasia (PIN) and CII were the significant independent predictors of PCa detection. PV (OR = 0.934) and CII (OR = 0.192) were both negative independent predictors. CII was a significant negative independent predictor in multivariate logistic regression models predicting the mean probability of PCa detection by age, PSA and PV. The inverse association of CII with PCa does not necessary mean protection because of PSA confounding.
参考文献 |
相关文章 |
计量指标
|
|
|
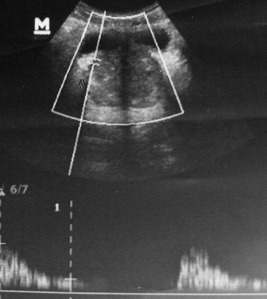
Implication of ultrasound bladder parameters on treatment response in patients with benign prostatic hyperplasia under medical management
Rajeev Thekumpadam Puthenveetil, Debajit Baishya, Sasanka Barua, Debanga Sarma
Asian Journal of Urology, 2015, 2(4): 233-237.
doi:10.1016/j.ajur.2015.08.004
摘要
(
421 )
PDF (1236KB)
(
445
)
Objective: The prevalence of benign prostatic hyperplasia (BPH) rapidly increases after the 4th decade of life. The combination of tamsulosin and dutasteride is a well established therapy for BPH of≥40 g. Non-invasive urodynamic parameters can predict the outcome of medical therapy in patients with BPH. We aimed to correlate these parameters with treatment responses in BPH patients under medical management. Methods: A prospective study was conducted in the Department of Urology in our hospital from May 2014 to April 2015. A total of 100 patients with BPH≥40 g who fulfilled our inclusion criteria were included. Treatment responses were determined by the International Prostate Symptom Score (IPSS) and uroflowmetry. Transabdominal ultrasonography with Doppler was performed to measure prostate volume, intravesical prostatic protrusion (IPP), detrusor wall thickness (DWT), the prostatic capsular artery resistive index (RI) and prostatic urethral angle (PUA) before and 3 months after combination therapy of tamsulosin and dutasteride. Treatment responses were correlated with non-invasive urodynamic parameters. Results: The IPSS, uroflow, age, prostate volume, RI, IPP, DWT and PUA were correlated before and after treatment. Of the 100 patients, 70 (70%) showed significant improvement and 30 (30%) showed no improvement with therapy. Conclusion: Ultrasound bladder parameters are useful tools for measuring the treatment response in BPH patients. Our study shows that RI and DWT significantly correlate with the treatment response in BPH patients. More importantly, pretreatment values of increased IPP and PUA determines the non-improvement of symptoms in BPH patients. Our study suggests the importance of transabdominal ultrasonography (KUB-P) with Doppler for evaluating treatment responses to medical management.
参考文献 |
相关文章 |
计量指标
|
|
|
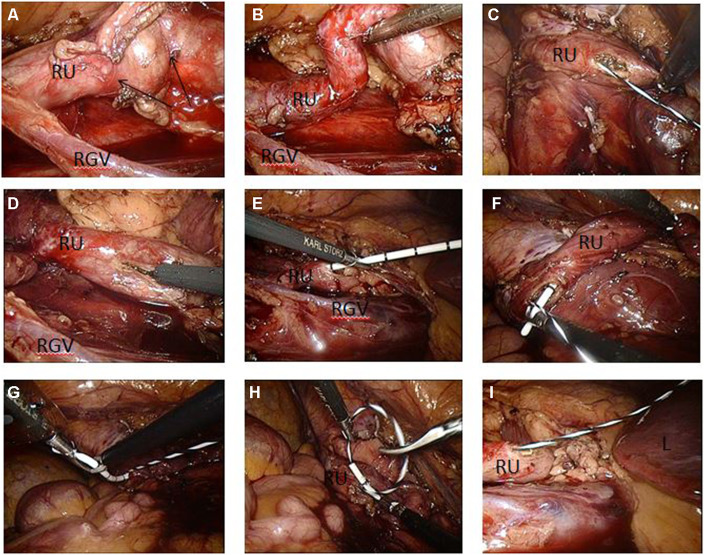
Laparoscopic ureterolysis with simultaneous ureteroscopy and percutaneous nephroscopy for treating complex ureteral obstruction after failed endoscopic intervention: A technical report
Zhixiang Wang, Bing Liu, Xiaofeng Gao, Yi Bao, Yang Wang, Huamao Ye, Yinghao Sun, Linhui Wang
Asian Journal of Urology, 2015, 2(4): 238-243.
doi:10.1016/j.ajur.2015.09.003
摘要
(
507 )
PDF (4374KB)
(
1086
)
Objective: Complex ureteral obstruction is refractory to conventional urological intervention. This report describes a case of laparoscopic ureterolysis with simultaneous ureteroscopy and percutaneous nephroscopy for treating complex ureteral obstruction. Methods: Right-side multiple ureteral stones and complicating ureteral obstruction failed an initial attempt of ureteroscopy lithotripsy with simultaneous percutaneous nephroscopy in a 23-year-old male. Laparoscopic ureterolysis with ureteroscopy and percutaneous nephroscopy was used simultaneously to dissect the periureteral adhesions with the patient placed in the Galdakao-modified supine Valdivia position. The ureter was incised to allow the insertion of a ureteral catheter through the twisted ureter, and a guide wire was advanced into the pelvis using ureteroscopy. A double-J stent was placed into the right-side ureter using antegrade percutaneous nephroscopy. Results: The laparoendoscopic procedure lasted 330 min with an estimated bleeding volume of 100 mL. The patient underwent an uneventful postoperative course, and postoperative followup radiography confirmed good positioning of the double-J stent. The double-J stent was removed 3 months after operation. The patient remained asymptomatic within a 13-month follow-up period.
参考文献 |
相关文章 |
计量指标
|
|
|
Stellate scar sign of renal cell carcinoma
Weibin Hou, Guanghua Liu, Zhigang Ji
Asian Journal of Urology, 2015, 2(4): 244-245.
doi:10.1016/j.ajur.2015.09.001
摘要
(
400 )
PDF (1703KB)
(
511
)
Stellate scar sign is defined as the centrally-placed, welldefined, stellate area of low density on computed tomography (CT) appearance of solid tumors. This kind of radiating enhancement from the center of the tumor, which is also referred as “a spoke-wheel-like enhancement” or central scar sign, usually has been recognized as a specific finding of renal oncocytoma. We describe a patient who developed clear cell renal cell carcinoma (RCC) displaying typical stellate scar sign on CT scans, which was confirmed by gross pathologic appearance.
参考文献 |
相关文章 |
计量指标
|
|





 当期目录
当期目录
